Na Zhang, Jingbo Shao, Hong Li, Jiashi Zhu, Min Xia, Kai Chen, Hui Jiang
{"title":"人源化cd19靶向CAR-T细胞治疗小儿复发/难治性急性淋巴细胞白血病伴CNSL或神经系统共病","authors":"Na Zhang, Jingbo Shao, Hong Li, Jiashi Zhu, Min Xia, Kai Chen, Hui Jiang","doi":"10.1097/CJI.0000000000000437","DOIUrl":null,"url":null,"abstract":"<p><p>Chimeric antigen receptor T cell (CAR-T) therapy has breakthrough potential for relapsed/refractory (R/R) acute lymphoblastic leukemia (ALL). However, because of the risk for neurotoxicity, trials usually exclude patients with central nervous system leukemia (CNSL) or active neurological comorbidities (NC). Here, we evaluated the efficacy and neurotoxicity of humanized CD19-directed CAR-T therapy for R/R ALL with CNSL or NC. Of 12 enrolled patients, 4 had CNSL with bone marrow (BM) or testicular recurrence, 3 had BM relapses with NC, and 5 had BM relapse without NC. Bridging chemotherapy was performed for high tumor burden before CAR-T therapy. Patients with CNSL or BM relapse with NC or without NC experienced 100% complete remission. Tumor burden reduction did not occur in 1 patient with NC, who developed grade 5 neurotoxicity before BM assessment, and one patient with CNSL developed leukoencephalopathy. Severe cytokine release syndrome and neurotoxicity developed in 0% with CNSL, 33.3% with BM relapse and NC, and 0% without NC. CAR-T cells expanded in the cerebrospinal fluid (CSF) of all patients with no difference among CNSL, BM with NC, or no NC (respective median percentages among lymphocyte: 33.7%, 48.2% and 34.5%, P =0.899; respective median concentrations: 0.82, 2.21, and 0.46/μL, P =0.719). Median CSF CAR-T cell duration was 5.5 (3-9) months with CNSL and 3 (2-3) months without CNSL ( P =0.031). CAR-T can be given safely and effectively to pediatric patients with R/R ALL with CNSL or NC who have near-normal neurological status. High tumor burden may confer increased risk for severe neurotoxicity.</p>","PeriodicalId":15996,"journal":{"name":"Journal of Immunotherapy","volume":"45 9","pages":"396-406"},"PeriodicalIF":3.2000,"publicationDate":"2022-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7e/44/cji-45-396.PMC9528944.pdf","citationCount":"0","resultStr":"{\"title\":\"Humanized CD19-directed CAR-T Cell Therapy in Pediatric Relapsed/Refractory Acute Lymphoblastic Leukemia With CNSL or Neurological Comorbidity.\",\"authors\":\"Na Zhang, Jingbo Shao, Hong Li, Jiashi Zhu, Min Xia, Kai Chen, Hui Jiang\",\"doi\":\"10.1097/CJI.0000000000000437\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Chimeric antigen receptor T cell (CAR-T) therapy has breakthrough potential for relapsed/refractory (R/R) acute lymphoblastic leukemia (ALL). However, because of the risk for neurotoxicity, trials usually exclude patients with central nervous system leukemia (CNSL) or active neurological comorbidities (NC). Here, we evaluated the efficacy and neurotoxicity of humanized CD19-directed CAR-T therapy for R/R ALL with CNSL or NC. Of 12 enrolled patients, 4 had CNSL with bone marrow (BM) or testicular recurrence, 3 had BM relapses with NC, and 5 had BM relapse without NC. Bridging chemotherapy was performed for high tumor burden before CAR-T therapy. Patients with CNSL or BM relapse with NC or without NC experienced 100% complete remission. Tumor burden reduction did not occur in 1 patient with NC, who developed grade 5 neurotoxicity before BM assessment, and one patient with CNSL developed leukoencephalopathy. Severe cytokine release syndrome and neurotoxicity developed in 0% with CNSL, 33.3% with BM relapse and NC, and 0% without NC. CAR-T cells expanded in the cerebrospinal fluid (CSF) of all patients with no difference among CNSL, BM with NC, or no NC (respective median percentages among lymphocyte: 33.7%, 48.2% and 34.5%, P =0.899; respective median concentrations: 0.82, 2.21, and 0.46/μL, P =0.719). Median CSF CAR-T cell duration was 5.5 (3-9) months with CNSL and 3 (2-3) months without CNSL ( P =0.031). CAR-T can be given safely and effectively to pediatric patients with R/R ALL with CNSL or NC who have near-normal neurological status. High tumor burden may confer increased risk for severe neurotoxicity.</p>\",\"PeriodicalId\":15996,\"journal\":{\"name\":\"Journal of Immunotherapy\",\"volume\":\"45 9\",\"pages\":\"396-406\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2022-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7e/44/cji-45-396.PMC9528944.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Immunotherapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/CJI.0000000000000437\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Immunotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/CJI.0000000000000437","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Humanized CD19-directed CAR-T Cell Therapy in Pediatric Relapsed/Refractory Acute Lymphoblastic Leukemia With CNSL or Neurological Comorbidity.
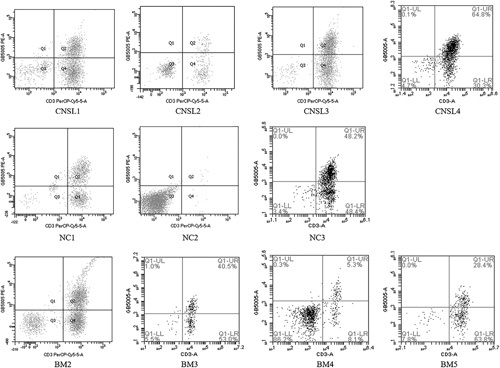
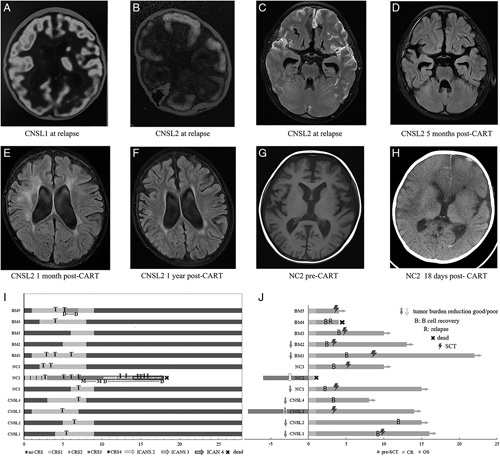
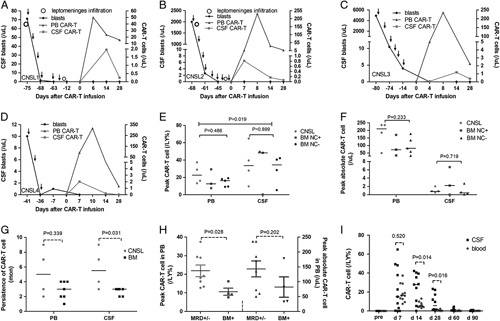
Chimeric antigen receptor T cell (CAR-T) therapy has breakthrough potential for relapsed/refractory (R/R) acute lymphoblastic leukemia (ALL). However, because of the risk for neurotoxicity, trials usually exclude patients with central nervous system leukemia (CNSL) or active neurological comorbidities (NC). Here, we evaluated the efficacy and neurotoxicity of humanized CD19-directed CAR-T therapy for R/R ALL with CNSL or NC. Of 12 enrolled patients, 4 had CNSL with bone marrow (BM) or testicular recurrence, 3 had BM relapses with NC, and 5 had BM relapse without NC. Bridging chemotherapy was performed for high tumor burden before CAR-T therapy. Patients with CNSL or BM relapse with NC or without NC experienced 100% complete remission. Tumor burden reduction did not occur in 1 patient with NC, who developed grade 5 neurotoxicity before BM assessment, and one patient with CNSL developed leukoencephalopathy. Severe cytokine release syndrome and neurotoxicity developed in 0% with CNSL, 33.3% with BM relapse and NC, and 0% without NC. CAR-T cells expanded in the cerebrospinal fluid (CSF) of all patients with no difference among CNSL, BM with NC, or no NC (respective median percentages among lymphocyte: 33.7%, 48.2% and 34.5%, P =0.899; respective median concentrations: 0.82, 2.21, and 0.46/μL, P =0.719). Median CSF CAR-T cell duration was 5.5 (3-9) months with CNSL and 3 (2-3) months without CNSL ( P =0.031). CAR-T can be given safely and effectively to pediatric patients with R/R ALL with CNSL or NC who have near-normal neurological status. High tumor burden may confer increased risk for severe neurotoxicity.
期刊介绍:
Journal of Immunotherapy features rapid publication of articles on immunomodulators, lymphokines, antibodies, cells, and cell products in cancer biology and therapy. Laboratory and preclinical studies, as well as investigative clinical reports, are presented. The journal emphasizes basic mechanisms and methods for the rapid transfer of technology from the laboratory to the clinic. JIT contains full-length articles, review articles, and short communications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


