Curry Sherard, Vineeth Sama, Jennie H Kwon, Khaled Shorbaji, Lauren V Huckaby, Brett A Welch, Chakradhari Inampudi, Ryan J Tedford, Arman Kilic
{"title":"老年受者心脏-肾脏联合移植的疗效。","authors":"Curry Sherard, Vineeth Sama, Jennie H Kwon, Khaled Shorbaji, Lauren V Huckaby, Brett A Welch, Chakradhari Inampudi, Ryan J Tedford, Arman Kilic","doi":"10.1155/2023/4528828","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The upper limit of recipient age for combined heart-kidney transplantation (HKT) remains controversial. This study evaluated the outcomes of HKT in patients aged ≥65 years.</p><p><strong>Methods: </strong>The United Network of Organ Sharing (UNOS) was used to identify patients undergoing HKT from 2005 to 2021. Patients were stratified by age at transplantation: <65 and ≥ 65 years. The primary outcome was one-year mortality. Secondary outcomes included 90-day and 5-year mortality, postoperative new-onset dialysis, postoperative stroke, acute rejection prior to discharge, and rejection within one-year of HKT. Survival was compared using Kaplan-Meier analysis, and risk adjustment for mortality was performed using Cox proportional hazards modeling.</p><p><strong>Results: </strong>HKT in recipients aged ≥65 significantly increased from 5.6% of all recipients in 2005 to 23.7% in 2021 (<i>p</i>=0.002). Of 2,022 HKT patients in the study period, 372 (18.40%) were aged ≥65. Older recipients were more likely to be male and white, and fewer required dialysis prior to HKT. There were no differences between cohorts in unadjusted 90-day, 1-year, or 5-year survival in Kaplan-Meier analysis. These findings persisted after risk-adjustment, with an adjusted hazard for one-year mortality for age ≥65 of 0.91 (95% CI (0.63-1.29), <i>p</i>=0.572). As a continuous variable, increasing age was not associated with one-year mortality (HR 1.01 (95% CI (1.00-1.02), <i>p</i>=0.236) per year). Patients aged ≥65 more frequently required new-onset dialysis prior to discharge (11.56% vs. 7.82%, <i>p</i>=0.051). Stroke and rejection rates were comparable.</p><p><strong>Conclusion: </strong>Combined HKT is increasing in older recipients, and advanced age ≥65 should not preclude HKT.</p>","PeriodicalId":9494,"journal":{"name":"Cardiology Research and Practice","volume":"2023 ","pages":"4528828"},"PeriodicalIF":1.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10314816/pdf/","citationCount":"1","resultStr":"{\"title\":\"Outcomes of Combined Heart-Kidney Transplantation in Older Recipients.\",\"authors\":\"Curry Sherard, Vineeth Sama, Jennie H Kwon, Khaled Shorbaji, Lauren V Huckaby, Brett A Welch, Chakradhari Inampudi, Ryan J Tedford, Arman Kilic\",\"doi\":\"10.1155/2023/4528828\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>The upper limit of recipient age for combined heart-kidney transplantation (HKT) remains controversial. This study evaluated the outcomes of HKT in patients aged ≥65 years.</p><p><strong>Methods: </strong>The United Network of Organ Sharing (UNOS) was used to identify patients undergoing HKT from 2005 to 2021. Patients were stratified by age at transplantation: <65 and ≥ 65 years. The primary outcome was one-year mortality. Secondary outcomes included 90-day and 5-year mortality, postoperative new-onset dialysis, postoperative stroke, acute rejection prior to discharge, and rejection within one-year of HKT. Survival was compared using Kaplan-Meier analysis, and risk adjustment for mortality was performed using Cox proportional hazards modeling.</p><p><strong>Results: </strong>HKT in recipients aged ≥65 significantly increased from 5.6% of all recipients in 2005 to 23.7% in 2021 (<i>p</i>=0.002). Of 2,022 HKT patients in the study period, 372 (18.40%) were aged ≥65. Older recipients were more likely to be male and white, and fewer required dialysis prior to HKT. There were no differences between cohorts in unadjusted 90-day, 1-year, or 5-year survival in Kaplan-Meier analysis. These findings persisted after risk-adjustment, with an adjusted hazard for one-year mortality for age ≥65 of 0.91 (95% CI (0.63-1.29), <i>p</i>=0.572). As a continuous variable, increasing age was not associated with one-year mortality (HR 1.01 (95% CI (1.00-1.02), <i>p</i>=0.236) per year). Patients aged ≥65 more frequently required new-onset dialysis prior to discharge (11.56% vs. 7.82%, <i>p</i>=0.051). Stroke and rejection rates were comparable.</p><p><strong>Conclusion: </strong>Combined HKT is increasing in older recipients, and advanced age ≥65 should not preclude HKT.</p>\",\"PeriodicalId\":9494,\"journal\":{\"name\":\"Cardiology Research and Practice\",\"volume\":\"2023 \",\"pages\":\"4528828\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10314816/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology Research and Practice\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1155/2023/4528828\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research and Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2023/4528828","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
摘要
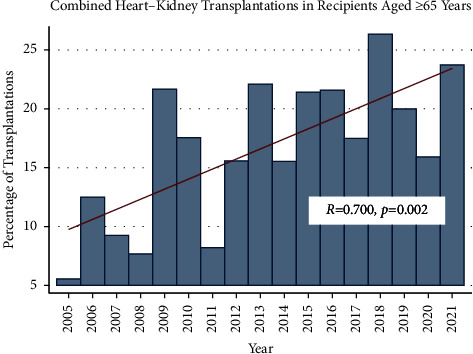
目的:心肾联合移植(HKT)的年龄上限仍有争议。本研究评估了年龄≥65岁患者的HKT预后。方法:使用联合器官共享网络(UNOS)对2005年至2021年接受HKT的患者进行识别。患者按移植年龄分层:结果:≥65岁受者的HKT从2005年的5.6%显著增加到2021年的23.7% (p=0.002)。在研究期间的2,022例HKT患者中,372例(18.40%)年龄≥65岁。年龄较大的接受者更可能是男性和白人,在HKT之前需要透析的人较少。在Kaplan-Meier分析中,未调整的90天、1年或5年生存率在队列之间没有差异。这些发现在风险调整后仍然存在,65岁以上人群一年死亡率的调整风险为0.91 (95% CI (0.63-1.29), p=0.572)。作为一个连续变量,年龄增加与一年死亡率无关(HR 1.01 (95% CI (1.00-1.02), p=0.236)。≥65岁的患者在出院前需要新发透析的频率更高(11.56% vs. 7.82%, p=0.051)。中风和排异率是相当的。结论:联合HKT在老年受者中增加,高龄≥65岁不应排除HKT。
Outcomes of Combined Heart-Kidney Transplantation in Older Recipients.
Objectives: The upper limit of recipient age for combined heart-kidney transplantation (HKT) remains controversial. This study evaluated the outcomes of HKT in patients aged ≥65 years.
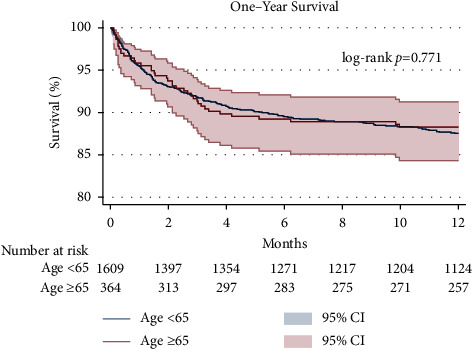
Methods: The United Network of Organ Sharing (UNOS) was used to identify patients undergoing HKT from 2005 to 2021. Patients were stratified by age at transplantation: <65 and ≥ 65 years. The primary outcome was one-year mortality. Secondary outcomes included 90-day and 5-year mortality, postoperative new-onset dialysis, postoperative stroke, acute rejection prior to discharge, and rejection within one-year of HKT. Survival was compared using Kaplan-Meier analysis, and risk adjustment for mortality was performed using Cox proportional hazards modeling.
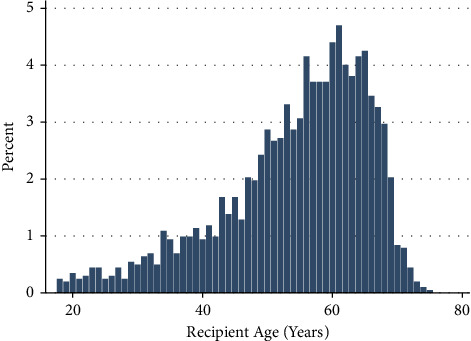
Results: HKT in recipients aged ≥65 significantly increased from 5.6% of all recipients in 2005 to 23.7% in 2021 (p=0.002). Of 2,022 HKT patients in the study period, 372 (18.40%) were aged ≥65. Older recipients were more likely to be male and white, and fewer required dialysis prior to HKT. There were no differences between cohorts in unadjusted 90-day, 1-year, or 5-year survival in Kaplan-Meier analysis. These findings persisted after risk-adjustment, with an adjusted hazard for one-year mortality for age ≥65 of 0.91 (95% CI (0.63-1.29), p=0.572). As a continuous variable, increasing age was not associated with one-year mortality (HR 1.01 (95% CI (1.00-1.02), p=0.236) per year). Patients aged ≥65 more frequently required new-onset dialysis prior to discharge (11.56% vs. 7.82%, p=0.051). Stroke and rejection rates were comparable.
Conclusion: Combined HKT is increasing in older recipients, and advanced age ≥65 should not preclude HKT.
期刊介绍:
Cardiology Research and Practice is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies that focus on the diagnosis and treatment of cardiovascular disease. The journal welcomes submissions related to systemic hypertension, arrhythmia, congestive heart failure, valvular heart disease, vascular disease, congenital heart disease, and cardiomyopathy.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


