Jose Arriola-Montenegro, Renato Beas, Renato Cerna-Viacava, Andres Chaponan-Lavalle, Karla Hernandez Randich, Diego Chambergo-Michilot, Herson Flores Sanga, Pornthira Mutirangura
{"title":"针对同时患有射血分数降低型心力衰竭和非酒精性脂肪肝患者的疗法。","authors":"Jose Arriola-Montenegro, Renato Beas, Renato Cerna-Viacava, Andres Chaponan-Lavalle, Karla Hernandez Randich, Diego Chambergo-Michilot, Herson Flores Sanga, Pornthira Mutirangura","doi":"10.4330/wjc.v15.i7.328","DOIUrl":null,"url":null,"abstract":"<p><p>Heart failure with reduced ejection fraction (HFrEF) and nonalcoholic fatty liver disease (NAFLD) are two common comorbidities that share similar pathophysiological mechanisms. There is a growing interest in the potential of targeted therapies to improve outcomes in patients with coexisting HFrEF and NAFLD. This manuscript reviews current and potential therapies for patients with coexisting HFrEF and NAFLD. Pharmacological therapies, including angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, mineralocorticoids receptor antagonist, and sodium-glucose cotransporter-2 inhibitors, have been shown to reduce fibrosis and fat deposits in the liver. However, there are currently no data showing the beneficial effects of sacubitril/valsartan, ivabradine, hydralazine, isosorbide nitrates, digoxin, or beta blockers on NAFLD in patients with HFrEF. This study highlights the importance of considering HFrEF and NAFLD when developing treatment plans for patients with these comorbidities. Further research is needed in patients with coexisting HFrEF and NAFLD, with an emphasis on novel therapies and the importance of a multidisciplinary approach for managing these complex comorbidities.</p>","PeriodicalId":23800,"journal":{"name":"World Journal of Cardiology","volume":null,"pages":null},"PeriodicalIF":1.9000,"publicationDate":"2023-07-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/00/97/WJC-15-328.PMC10415861.pdf","citationCount":"0","resultStr":"{\"title\":\"Therapies for patients with coexisting heart failure with reduced ejection fraction and non-alcoholic fatty liver disease.\",\"authors\":\"Jose Arriola-Montenegro, Renato Beas, Renato Cerna-Viacava, Andres Chaponan-Lavalle, Karla Hernandez Randich, Diego Chambergo-Michilot, Herson Flores Sanga, Pornthira Mutirangura\",\"doi\":\"10.4330/wjc.v15.i7.328\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Heart failure with reduced ejection fraction (HFrEF) and nonalcoholic fatty liver disease (NAFLD) are two common comorbidities that share similar pathophysiological mechanisms. There is a growing interest in the potential of targeted therapies to improve outcomes in patients with coexisting HFrEF and NAFLD. This manuscript reviews current and potential therapies for patients with coexisting HFrEF and NAFLD. Pharmacological therapies, including angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, mineralocorticoids receptor antagonist, and sodium-glucose cotransporter-2 inhibitors, have been shown to reduce fibrosis and fat deposits in the liver. However, there are currently no data showing the beneficial effects of sacubitril/valsartan, ivabradine, hydralazine, isosorbide nitrates, digoxin, or beta blockers on NAFLD in patients with HFrEF. This study highlights the importance of considering HFrEF and NAFLD when developing treatment plans for patients with these comorbidities. Further research is needed in patients with coexisting HFrEF and NAFLD, with an emphasis on novel therapies and the importance of a multidisciplinary approach for managing these complex comorbidities.</p>\",\"PeriodicalId\":23800,\"journal\":{\"name\":\"World Journal of Cardiology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2023-07-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/00/97/WJC-15-328.PMC10415861.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4330/wjc.v15.i7.328\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4330/wjc.v15.i7.328","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Therapies for patients with coexisting heart failure with reduced ejection fraction and non-alcoholic fatty liver disease.
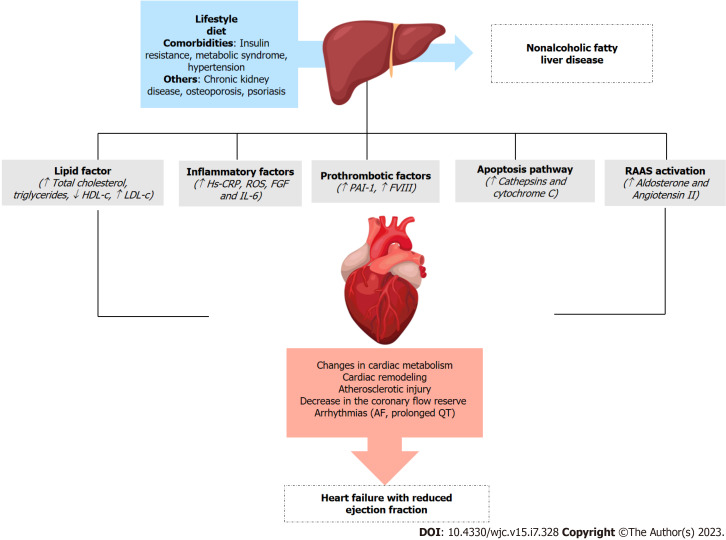
Heart failure with reduced ejection fraction (HFrEF) and nonalcoholic fatty liver disease (NAFLD) are two common comorbidities that share similar pathophysiological mechanisms. There is a growing interest in the potential of targeted therapies to improve outcomes in patients with coexisting HFrEF and NAFLD. This manuscript reviews current and potential therapies for patients with coexisting HFrEF and NAFLD. Pharmacological therapies, including angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, mineralocorticoids receptor antagonist, and sodium-glucose cotransporter-2 inhibitors, have been shown to reduce fibrosis and fat deposits in the liver. However, there are currently no data showing the beneficial effects of sacubitril/valsartan, ivabradine, hydralazine, isosorbide nitrates, digoxin, or beta blockers on NAFLD in patients with HFrEF. This study highlights the importance of considering HFrEF and NAFLD when developing treatment plans for patients with these comorbidities. Further research is needed in patients with coexisting HFrEF and NAFLD, with an emphasis on novel therapies and the importance of a multidisciplinary approach for managing these complex comorbidities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


