Lyndsey L Fournier, ErinMarie O Kimbrough, Muhamad Alhaj Moustafa, Ke Li, Madiha Iqbal, Vivek Gupta, Han W Tun
{"title":"以中枢为中心的治疗成功治疗多发复发继发性中枢非生发中心弥漫性大b细胞淋巴瘤。","authors":"Lyndsey L Fournier, ErinMarie O Kimbrough, Muhamad Alhaj Moustafa, Ke Li, Madiha Iqbal, Vivek Gupta, Han W Tun","doi":"10.2147/JBM.S405521","DOIUrl":null,"url":null,"abstract":"<p><p>Secondary central nervous system involvement by systemic diffuse large B-cell lymphoma (DLBCL) carries a very poor prognosis. We present a female patient who had two episodes of intracerebral central nervous system (CNS)-only relapse of systemic non-germinal center diffuse large B-cell lymphoma (NGC-DLBCL). Her treatment at initial diagnosis consisted of induction with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) and intrathecal (IT) - methotrexate (MTX) followed by consolidation with autologous stem cell transplant (ASCT) after high-dose carmustine, etoposide, cytarabine, and melphalan (BEAM) chemotherapy. She had the first CNS-only relapse 1.5 years post-ASCT and received whole brain radiation therapy (WBRT). She developed the second intracerebral CNS-only relapse 2 years post-WBRT. A CNS-centric therapeutic approach with salvage chemoimmunotherapy incorporating rituximab, high-dose methotrexate (HD-MTX), high-dose cytarabine (HiDAC), and ibrutinib was utilized for her second CNS-only relapse. She underwent consolidation with a second ASCT following high-dose carmustine (BCNU) and thiotepa chemotherapy. Given her high risk of CNS recurrence, she was started on maintenance ibrutinib. To date, she has remained in complete remission for 3 years. In our experience, multiply relapsed secondary CNS lymphoma (SCNSL) with this response is very rare. We suggest one CNS-centric therapeutic approach that can potentially salvage patients with SCNSL who have not had prior exposure to adequate CNS-directed therapies but acknowledge that additional research is necessary to validate our findings.</p>","PeriodicalId":15166,"journal":{"name":"Journal of Blood Medicine","volume":"14 ","pages":"455-461"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/14/3b/jbm-14-455.PMC10440079.pdf","citationCount":"0","resultStr":"{\"title\":\"Multiply Relapsed Secondary CNS Non-Germinal Center Diffuse Large B-Cell Lymphoma Successfully Treated with CNS-Centric Therapy.\",\"authors\":\"Lyndsey L Fournier, ErinMarie O Kimbrough, Muhamad Alhaj Moustafa, Ke Li, Madiha Iqbal, Vivek Gupta, Han W Tun\",\"doi\":\"10.2147/JBM.S405521\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Secondary central nervous system involvement by systemic diffuse large B-cell lymphoma (DLBCL) carries a very poor prognosis. We present a female patient who had two episodes of intracerebral central nervous system (CNS)-only relapse of systemic non-germinal center diffuse large B-cell lymphoma (NGC-DLBCL). Her treatment at initial diagnosis consisted of induction with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) and intrathecal (IT) - methotrexate (MTX) followed by consolidation with autologous stem cell transplant (ASCT) after high-dose carmustine, etoposide, cytarabine, and melphalan (BEAM) chemotherapy. She had the first CNS-only relapse 1.5 years post-ASCT and received whole brain radiation therapy (WBRT). She developed the second intracerebral CNS-only relapse 2 years post-WBRT. A CNS-centric therapeutic approach with salvage chemoimmunotherapy incorporating rituximab, high-dose methotrexate (HD-MTX), high-dose cytarabine (HiDAC), and ibrutinib was utilized for her second CNS-only relapse. She underwent consolidation with a second ASCT following high-dose carmustine (BCNU) and thiotepa chemotherapy. Given her high risk of CNS recurrence, she was started on maintenance ibrutinib. To date, she has remained in complete remission for 3 years. In our experience, multiply relapsed secondary CNS lymphoma (SCNSL) with this response is very rare. We suggest one CNS-centric therapeutic approach that can potentially salvage patients with SCNSL who have not had prior exposure to adequate CNS-directed therapies but acknowledge that additional research is necessary to validate our findings.</p>\",\"PeriodicalId\":15166,\"journal\":{\"name\":\"Journal of Blood Medicine\",\"volume\":\"14 \",\"pages\":\"455-461\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/14/3b/jbm-14-455.PMC10440079.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Blood Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/JBM.S405521\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Blood Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/JBM.S405521","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Multiply Relapsed Secondary CNS Non-Germinal Center Diffuse Large B-Cell Lymphoma Successfully Treated with CNS-Centric Therapy.
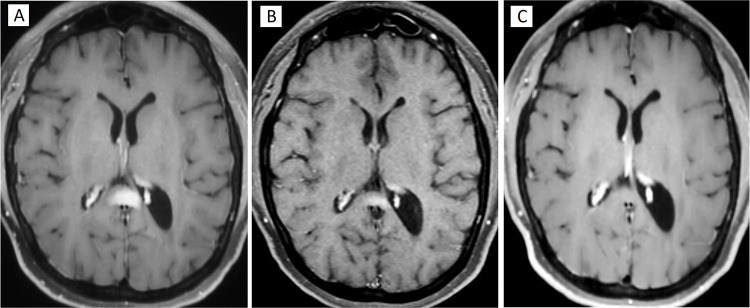
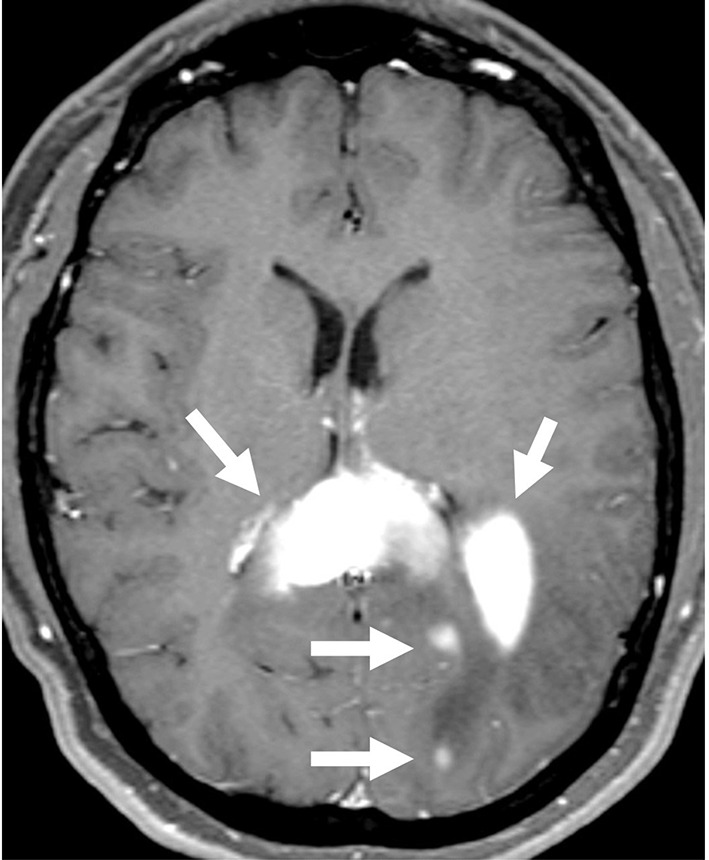
Secondary central nervous system involvement by systemic diffuse large B-cell lymphoma (DLBCL) carries a very poor prognosis. We present a female patient who had two episodes of intracerebral central nervous system (CNS)-only relapse of systemic non-germinal center diffuse large B-cell lymphoma (NGC-DLBCL). Her treatment at initial diagnosis consisted of induction with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) and intrathecal (IT) - methotrexate (MTX) followed by consolidation with autologous stem cell transplant (ASCT) after high-dose carmustine, etoposide, cytarabine, and melphalan (BEAM) chemotherapy. She had the first CNS-only relapse 1.5 years post-ASCT and received whole brain radiation therapy (WBRT). She developed the second intracerebral CNS-only relapse 2 years post-WBRT. A CNS-centric therapeutic approach with salvage chemoimmunotherapy incorporating rituximab, high-dose methotrexate (HD-MTX), high-dose cytarabine (HiDAC), and ibrutinib was utilized for her second CNS-only relapse. She underwent consolidation with a second ASCT following high-dose carmustine (BCNU) and thiotepa chemotherapy. Given her high risk of CNS recurrence, she was started on maintenance ibrutinib. To date, she has remained in complete remission for 3 years. In our experience, multiply relapsed secondary CNS lymphoma (SCNSL) with this response is very rare. We suggest one CNS-centric therapeutic approach that can potentially salvage patients with SCNSL who have not had prior exposure to adequate CNS-directed therapies but acknowledge that additional research is necessary to validate our findings.
期刊介绍:
The Journal of Blood Medicine is an international, peer-reviewed, open access, online journal publishing laboratory, experimental and clinical aspects of all topics pertaining to blood based medicine including but not limited to: Transfusion Medicine (blood components, stem cell transplantation, apheresis, gene based therapeutics), Blood collection, Donor issues, Transmittable diseases, and Blood banking logistics, Immunohematology, Artificial and alternative blood based therapeutics, Hematology including disorders/pathology related to leukocytes/immunology, red cells, platelets and hemostasis, Biotechnology/nanotechnology of blood related medicine, Legal aspects of blood medicine, Historical perspectives. Original research, short reports, reviews, case reports and commentaries are invited.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


