Andre Briosa E Gala, Michael Timothy Brian Pope, Milena Leo, Alexander James Sharp, Victor Tsoi, John Paisey, Nick Curzen, Timothy Rider Betts
{"title":"每日心律监测指导下的“口袋药丸”口服抗凝治疗对房颤患者脑卒中预防:一项系统综述和荟萃分析","authors":"Andre Briosa E Gala, Michael Timothy Brian Pope, Milena Leo, Alexander James Sharp, Victor Tsoi, John Paisey, Nick Curzen, Timothy Rider Betts","doi":"10.15420/aer.2022.22","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>In patients with a low AF burden and long periods of sinus rhythm, 'pill-in-the-pocket' oral anticoagulation (OAC) may, taken as needed in response to AF episodes, offer the same thromboembolic protection as continuous, life-long OAC, while reducing bleeding complications at the same time. The purpose of this study is to systematically summarise available evidence pertaining to the feasibility, safety and efficacy of pill-in-the-pocket OAC.</p><p><strong>Methods: </strong>Medline and Embase were searched from inception to July 2022 for studies adopting a pill-in-the-pocket OAC strategy in AF patients guided by daily rhythm monitoring (PROSPERO/CRD42020209564). Outcomes of interest were extracted and event rates per patient-years of follow-up were calculated. A random effects model was used for pooled estimates.</p><p><strong>Results: </strong>Eight studies were included (711 patients). Daily rhythm monitoring was continuous in six studies and intermittent in two (pulse checks or smartphone single-lead electrocardiograms were used). Anticoagulation criteria varied across studies, reflecting the uncertainty regarding the AF burden that warrants anticoagulation. The mean time from AF meeting OAC criteria to its initiation was not reported. Adopting pill-in-the-pocket OAC led to 390 (54.7%) patients stopping OAC, 85 (12.0%) patients taking pill-in-the-pocket OAC and 237 (33.3%) patients remaining on or returning to continuous OAC. Overall, annualised ischaemic stroke and major bleeding rates per patient-year of follow-up were low at 0.005 (95% CI [0.002-0.012]) and 0.024 (95% CI [0.013-0.043]), respectively.</p><p><strong>Conclusion: </strong>Current evidence, although encouraging, is insufficient to inform practice. Additional studies are required to improve our understanding of the relationships between AF burden and thromboembolic risk to help define anticoagulation criteria and appropriate monitoring strategies.</p>","PeriodicalId":8412,"journal":{"name":"Arrhythmia & Electrophysiology Review","volume":"12 ","pages":"e05"},"PeriodicalIF":3.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/af/03/aer-12-e05.PMC10433111.pdf","citationCount":"0","resultStr":"{\"title\":\"'Pill-in-the-pocket' Oral Anticoagulation Guided by Daily Rhythm Monitoring for Stroke Prevention in Patients with AF: A Systematic Review and Meta-analysis.\",\"authors\":\"Andre Briosa E Gala, Michael Timothy Brian Pope, Milena Leo, Alexander James Sharp, Victor Tsoi, John Paisey, Nick Curzen, Timothy Rider Betts\",\"doi\":\"10.15420/aer.2022.22\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>In patients with a low AF burden and long periods of sinus rhythm, 'pill-in-the-pocket' oral anticoagulation (OAC) may, taken as needed in response to AF episodes, offer the same thromboembolic protection as continuous, life-long OAC, while reducing bleeding complications at the same time. The purpose of this study is to systematically summarise available evidence pertaining to the feasibility, safety and efficacy of pill-in-the-pocket OAC.</p><p><strong>Methods: </strong>Medline and Embase were searched from inception to July 2022 for studies adopting a pill-in-the-pocket OAC strategy in AF patients guided by daily rhythm monitoring (PROSPERO/CRD42020209564). Outcomes of interest were extracted and event rates per patient-years of follow-up were calculated. A random effects model was used for pooled estimates.</p><p><strong>Results: </strong>Eight studies were included (711 patients). Daily rhythm monitoring was continuous in six studies and intermittent in two (pulse checks or smartphone single-lead electrocardiograms were used). Anticoagulation criteria varied across studies, reflecting the uncertainty regarding the AF burden that warrants anticoagulation. The mean time from AF meeting OAC criteria to its initiation was not reported. Adopting pill-in-the-pocket OAC led to 390 (54.7%) patients stopping OAC, 85 (12.0%) patients taking pill-in-the-pocket OAC and 237 (33.3%) patients remaining on or returning to continuous OAC. Overall, annualised ischaemic stroke and major bleeding rates per patient-year of follow-up were low at 0.005 (95% CI [0.002-0.012]) and 0.024 (95% CI [0.013-0.043]), respectively.</p><p><strong>Conclusion: </strong>Current evidence, although encouraging, is insufficient to inform practice. Additional studies are required to improve our understanding of the relationships between AF burden and thromboembolic risk to help define anticoagulation criteria and appropriate monitoring strategies.</p>\",\"PeriodicalId\":8412,\"journal\":{\"name\":\"Arrhythmia & Electrophysiology Review\",\"volume\":\"12 \",\"pages\":\"e05\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/af/03/aer-12-e05.PMC10433111.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Arrhythmia & Electrophysiology Review\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.15420/aer.2022.22\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arrhythmia & Electrophysiology Review","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15420/aer.2022.22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
'Pill-in-the-pocket' Oral Anticoagulation Guided by Daily Rhythm Monitoring for Stroke Prevention in Patients with AF: A Systematic Review and Meta-analysis.
Aims: In patients with a low AF burden and long periods of sinus rhythm, 'pill-in-the-pocket' oral anticoagulation (OAC) may, taken as needed in response to AF episodes, offer the same thromboembolic protection as continuous, life-long OAC, while reducing bleeding complications at the same time. The purpose of this study is to systematically summarise available evidence pertaining to the feasibility, safety and efficacy of pill-in-the-pocket OAC.
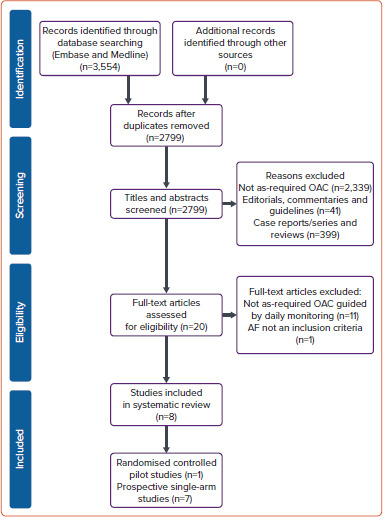
Methods: Medline and Embase were searched from inception to July 2022 for studies adopting a pill-in-the-pocket OAC strategy in AF patients guided by daily rhythm monitoring (PROSPERO/CRD42020209564). Outcomes of interest were extracted and event rates per patient-years of follow-up were calculated. A random effects model was used for pooled estimates.
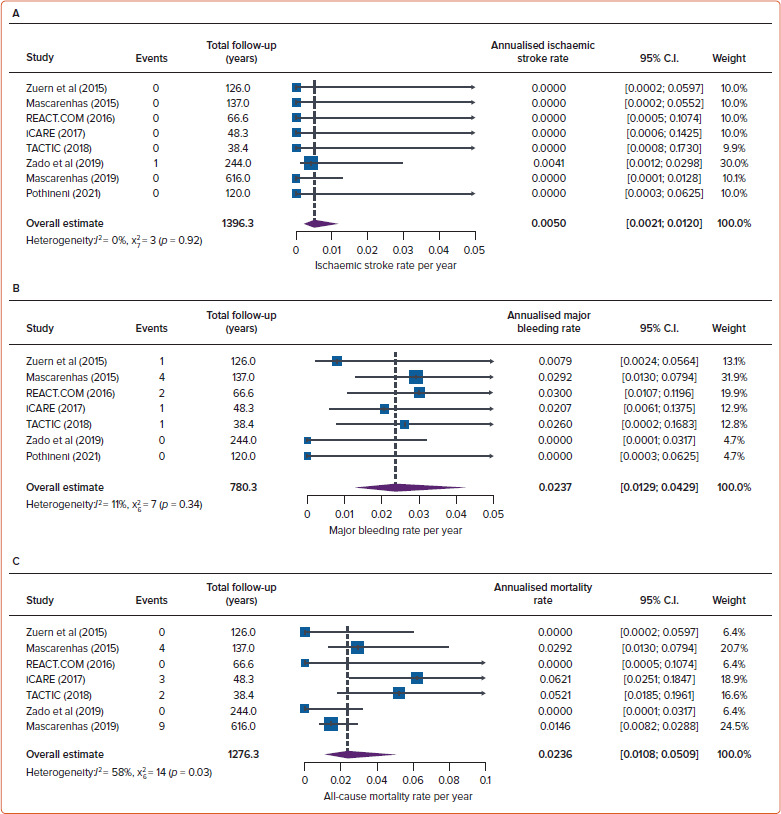
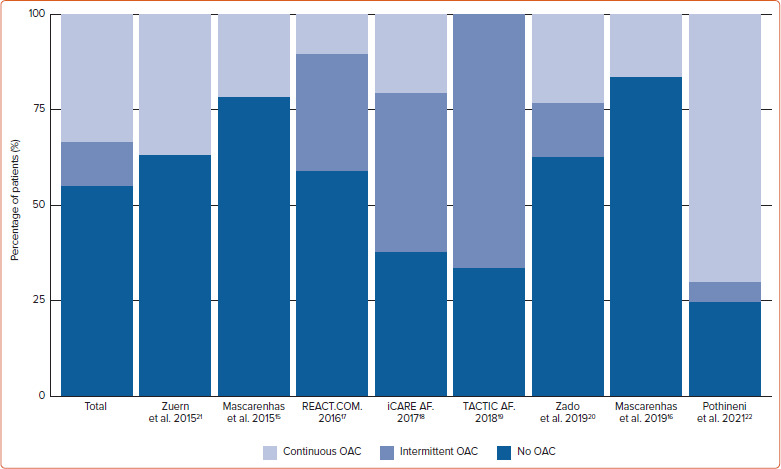
Results: Eight studies were included (711 patients). Daily rhythm monitoring was continuous in six studies and intermittent in two (pulse checks or smartphone single-lead electrocardiograms were used). Anticoagulation criteria varied across studies, reflecting the uncertainty regarding the AF burden that warrants anticoagulation. The mean time from AF meeting OAC criteria to its initiation was not reported. Adopting pill-in-the-pocket OAC led to 390 (54.7%) patients stopping OAC, 85 (12.0%) patients taking pill-in-the-pocket OAC and 237 (33.3%) patients remaining on or returning to continuous OAC. Overall, annualised ischaemic stroke and major bleeding rates per patient-year of follow-up were low at 0.005 (95% CI [0.002-0.012]) and 0.024 (95% CI [0.013-0.043]), respectively.
Conclusion: Current evidence, although encouraging, is insufficient to inform practice. Additional studies are required to improve our understanding of the relationships between AF burden and thromboembolic risk to help define anticoagulation criteria and appropriate monitoring strategies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


