Barresi Nv, S McCollum, E Faherty, J M Steele, R Karnik
{"title":"mRNA COVID-19 疫苗接种后心肌炎患者左心室功能的纵向评估","authors":"Barresi Nv, S McCollum, E Faherty, J M Steele, R Karnik","doi":"10.1007/s00246-023-03200-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Multiple reports have described myopericarditis following mRNA COVID-19 vaccination. However, data on the persistence of subclinical myocardial injury assessed by left ventricular (LV) longitudinal strain (LVLS) is limited.</p><p><strong>Objectives: </strong>Our aim was to assess LV function longitudinally in our cohort of COVID-19 vaccine-related myopericarditis using ejection fraction (EF), fractional shortening (FS), LVLS, and diastolic parameters.</p><p><strong>Methods: </strong>Retrospective, single-center review of demographic, laboratory, and management data was performed on 20 patients meeting diagnostic criteria for myopericarditis after mRNA COVID-19 vaccination. Echocardiographic images were obtained on initial presentation (time 0), at a median of 12 days (7.5, 18.5; time 1), and at a median of 44 days (29.5, 83.5; time 2). FS was calculated by M-mode, EF by 5/6 area-length methods, LVLS by utilization of TOMTEC software, and diastolic function by tissue Doppler. All parameters were compared across pairs of these time points using Wilcoxon signed-rank test.</p><p><strong>Results: </strong>Our cohort consisted predominantly of adolescent males (85%) with mild presentation of myopericarditis. The median EF was 61.6% (54.6, 68.0), 63.8% (60.7, 68.3), 61.4% (60.1, 64.6) at times 0, 1, and 2, respectively. Upon initial presentation, 47% of our cohort had LVLS < -18%. The median LVLS was -18.6% (-16.9, -21.0) at time 0, -21.2% at time 1 (-19.4, -23.5) (p = 0.004) and -20.8% (-18.7, -21.7) at time 2 (p = 0.004, as compared to time 0).</p><p><strong>Conclusions: </strong>Though many of our patients had abnormal strain during acute illness, LVLS improved longitudinally, indicating myocardial recovery. LVLS can be used as marker of subclinical myocardial injury and risk stratification in this population.</p>","PeriodicalId":19814,"journal":{"name":"Pediatric Cardiology","volume":" ","pages":"1524-1532"},"PeriodicalIF":1.4000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10251331/pdf/","citationCount":"0","resultStr":"{\"title\":\"Longitudinal Assessment of Left Ventricular Function in Patients with Myopericarditis After mRNA COVID-19 Vaccination.\",\"authors\":\"Barresi Nv, S McCollum, E Faherty, J M Steele, R Karnik\",\"doi\":\"10.1007/s00246-023-03200-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Multiple reports have described myopericarditis following mRNA COVID-19 vaccination. However, data on the persistence of subclinical myocardial injury assessed by left ventricular (LV) longitudinal strain (LVLS) is limited.</p><p><strong>Objectives: </strong>Our aim was to assess LV function longitudinally in our cohort of COVID-19 vaccine-related myopericarditis using ejection fraction (EF), fractional shortening (FS), LVLS, and diastolic parameters.</p><p><strong>Methods: </strong>Retrospective, single-center review of demographic, laboratory, and management data was performed on 20 patients meeting diagnostic criteria for myopericarditis after mRNA COVID-19 vaccination. Echocardiographic images were obtained on initial presentation (time 0), at a median of 12 days (7.5, 18.5; time 1), and at a median of 44 days (29.5, 83.5; time 2). FS was calculated by M-mode, EF by 5/6 area-length methods, LVLS by utilization of TOMTEC software, and diastolic function by tissue Doppler. All parameters were compared across pairs of these time points using Wilcoxon signed-rank test.</p><p><strong>Results: </strong>Our cohort consisted predominantly of adolescent males (85%) with mild presentation of myopericarditis. The median EF was 61.6% (54.6, 68.0), 63.8% (60.7, 68.3), 61.4% (60.1, 64.6) at times 0, 1, and 2, respectively. Upon initial presentation, 47% of our cohort had LVLS < -18%. The median LVLS was -18.6% (-16.9, -21.0) at time 0, -21.2% at time 1 (-19.4, -23.5) (p = 0.004) and -20.8% (-18.7, -21.7) at time 2 (p = 0.004, as compared to time 0).</p><p><strong>Conclusions: </strong>Though many of our patients had abnormal strain during acute illness, LVLS improved longitudinally, indicating myocardial recovery. LVLS can be used as marker of subclinical myocardial injury and risk stratification in this population.</p>\",\"PeriodicalId\":19814,\"journal\":{\"name\":\"Pediatric Cardiology\",\"volume\":\" \",\"pages\":\"1524-1532\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10251331/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00246-023-03200-2\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/6/9 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00246-023-03200-2","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/9 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Longitudinal Assessment of Left Ventricular Function in Patients with Myopericarditis After mRNA COVID-19 Vaccination.
Background: Multiple reports have described myopericarditis following mRNA COVID-19 vaccination. However, data on the persistence of subclinical myocardial injury assessed by left ventricular (LV) longitudinal strain (LVLS) is limited.
Objectives: Our aim was to assess LV function longitudinally in our cohort of COVID-19 vaccine-related myopericarditis using ejection fraction (EF), fractional shortening (FS), LVLS, and diastolic parameters.
Methods: Retrospective, single-center review of demographic, laboratory, and management data was performed on 20 patients meeting diagnostic criteria for myopericarditis after mRNA COVID-19 vaccination. Echocardiographic images were obtained on initial presentation (time 0), at a median of 12 days (7.5, 18.5; time 1), and at a median of 44 days (29.5, 83.5; time 2). FS was calculated by M-mode, EF by 5/6 area-length methods, LVLS by utilization of TOMTEC software, and diastolic function by tissue Doppler. All parameters were compared across pairs of these time points using Wilcoxon signed-rank test.
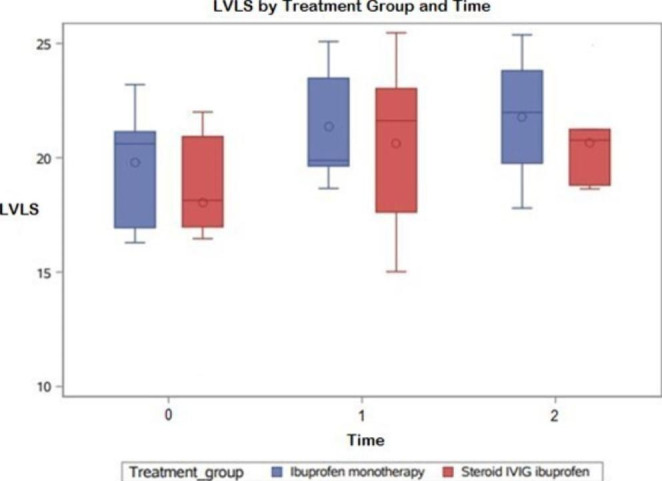
Results: Our cohort consisted predominantly of adolescent males (85%) with mild presentation of myopericarditis. The median EF was 61.6% (54.6, 68.0), 63.8% (60.7, 68.3), 61.4% (60.1, 64.6) at times 0, 1, and 2, respectively. Upon initial presentation, 47% of our cohort had LVLS < -18%. The median LVLS was -18.6% (-16.9, -21.0) at time 0, -21.2% at time 1 (-19.4, -23.5) (p = 0.004) and -20.8% (-18.7, -21.7) at time 2 (p = 0.004, as compared to time 0).
Conclusions: Though many of our patients had abnormal strain during acute illness, LVLS improved longitudinally, indicating myocardial recovery. LVLS can be used as marker of subclinical myocardial injury and risk stratification in this population.
期刊介绍:
The editor of Pediatric Cardiology welcomes original manuscripts concerning all aspects of heart disease in infants, children, and adolescents, including embryology and anatomy, physiology and pharmacology, biochemistry, pathology, genetics, radiology, clinical aspects, investigative cardiology, electrophysiology and echocardiography, and cardiac surgery. Articles which may include original articles, review articles, letters to the editor etc., must be written in English and must be submitted solely to Pediatric Cardiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


