{"title":"无法手术的转移分化性甲状腺癌的第一击个性化预测放射性碘处方。","authors":"Yung Hsiang Kao","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The traditional practice of empiric radioiodine (I-131) prescription is scientifically obsolete and inappropriate for inoperable metastatic differentiated thyroid cancer. However, theranostically guided prescription is still years away for many institutions. A personalized predictive method of radioiodine prescription that bridges the gap between empiric and theranostic methods is presented. It is an adaptation of the \"maximum tolerated activity\" method, where serial blood sampling is replaced by population kinetics carefully chosen by the user. It aims to maximize crossfire benefits within safety constraints to overcome tumour absorbed dose heterogeneity for a safe and effective first radioiodine fraction i.e., the First Strike.</p><p><strong>Methods: </strong>The EANM method of blood dosimetry was incorporated with population kinetics, marrow and lung safety constraints, body habitus and clinical assessment of metastatic extent. Population data of whole body and blood kinetics in patients with and without metastases, prepared by recombinant human thyroid stimulating hormone or thyroid hormone withdrawal, and the maximum safe marrow dose rate were deduced from published data. For diffuse lung metastases, the lung safety limit was linearly scaled by height and separated into lung and remainder-of-body components.</p><p><strong>Results: </strong>The slowest whole body Time Integrated Activity Coefficient (TIAC) amongst patients with any metastases was 33.5±17.0 h and the highest percentage of whole body TIAC attributed to blood was 16.6±7.9%, prepared by thyroid hormone withdrawal. A variety of other average radioiodine kinetics is tabulated. Maximum safe marrow dose rate was deduced to be 0.265 Gy/h per fraction, where blood TIAC is normalised to administered activity. An easy-to-use calculator was developed which only requires height, weight and gender to populate recommendations for personalized First Strike prescription. The user decides by clinical gestalt whether the prescription is to be constrained by marrow or lung, then selects an activity depending on how extensive the metastases are likely to be. A Standard Female with oligometastasis and good urine output without diffuse lung metastasis is expected to safely tolerate 8.03 GBq of radioiodine as the First Strike.</p><p><strong>Conclusion: </strong>This predictive method will help institutions rationalise the First Strike prescription based on radiobiologically sound principles, personalised to individual circumstances.</p>","PeriodicalId":8503,"journal":{"name":"Asia Oceania Journal of Nuclear Medicine and Biology","volume":null,"pages":null},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10261697/pdf/","citationCount":"0","resultStr":"{\"title\":\"First Strike personalized predictive radioiodine prescription for inoperable metastatic differentiated thyroid cancer.\",\"authors\":\"Yung Hsiang Kao\",\"doi\":\"\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>The traditional practice of empiric radioiodine (I-131) prescription is scientifically obsolete and inappropriate for inoperable metastatic differentiated thyroid cancer. However, theranostically guided prescription is still years away for many institutions. A personalized predictive method of radioiodine prescription that bridges the gap between empiric and theranostic methods is presented. It is an adaptation of the \\\"maximum tolerated activity\\\" method, where serial blood sampling is replaced by population kinetics carefully chosen by the user. It aims to maximize crossfire benefits within safety constraints to overcome tumour absorbed dose heterogeneity for a safe and effective first radioiodine fraction i.e., the First Strike.</p><p><strong>Methods: </strong>The EANM method of blood dosimetry was incorporated with population kinetics, marrow and lung safety constraints, body habitus and clinical assessment of metastatic extent. Population data of whole body and blood kinetics in patients with and without metastases, prepared by recombinant human thyroid stimulating hormone or thyroid hormone withdrawal, and the maximum safe marrow dose rate were deduced from published data. For diffuse lung metastases, the lung safety limit was linearly scaled by height and separated into lung and remainder-of-body components.</p><p><strong>Results: </strong>The slowest whole body Time Integrated Activity Coefficient (TIAC) amongst patients with any metastases was 33.5±17.0 h and the highest percentage of whole body TIAC attributed to blood was 16.6±7.9%, prepared by thyroid hormone withdrawal. A variety of other average radioiodine kinetics is tabulated. Maximum safe marrow dose rate was deduced to be 0.265 Gy/h per fraction, where blood TIAC is normalised to administered activity. An easy-to-use calculator was developed which only requires height, weight and gender to populate recommendations for personalized First Strike prescription. The user decides by clinical gestalt whether the prescription is to be constrained by marrow or lung, then selects an activity depending on how extensive the metastases are likely to be. A Standard Female with oligometastasis and good urine output without diffuse lung metastasis is expected to safely tolerate 8.03 GBq of radioiodine as the First Strike.</p><p><strong>Conclusion: </strong>This predictive method will help institutions rationalise the First Strike prescription based on radiobiologically sound principles, personalised to individual circumstances.</p>\",\"PeriodicalId\":8503,\"journal\":{\"name\":\"Asia Oceania Journal of Nuclear Medicine and Biology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10261697/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Asia Oceania Journal of Nuclear Medicine and Biology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asia Oceania Journal of Nuclear Medicine and Biology","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
First Strike personalized predictive radioiodine prescription for inoperable metastatic differentiated thyroid cancer.
Objectives: The traditional practice of empiric radioiodine (I-131) prescription is scientifically obsolete and inappropriate for inoperable metastatic differentiated thyroid cancer. However, theranostically guided prescription is still years away for many institutions. A personalized predictive method of radioiodine prescription that bridges the gap between empiric and theranostic methods is presented. It is an adaptation of the "maximum tolerated activity" method, where serial blood sampling is replaced by population kinetics carefully chosen by the user. It aims to maximize crossfire benefits within safety constraints to overcome tumour absorbed dose heterogeneity for a safe and effective first radioiodine fraction i.e., the First Strike.
Methods: The EANM method of blood dosimetry was incorporated with population kinetics, marrow and lung safety constraints, body habitus and clinical assessment of metastatic extent. Population data of whole body and blood kinetics in patients with and without metastases, prepared by recombinant human thyroid stimulating hormone or thyroid hormone withdrawal, and the maximum safe marrow dose rate were deduced from published data. For diffuse lung metastases, the lung safety limit was linearly scaled by height and separated into lung and remainder-of-body components.
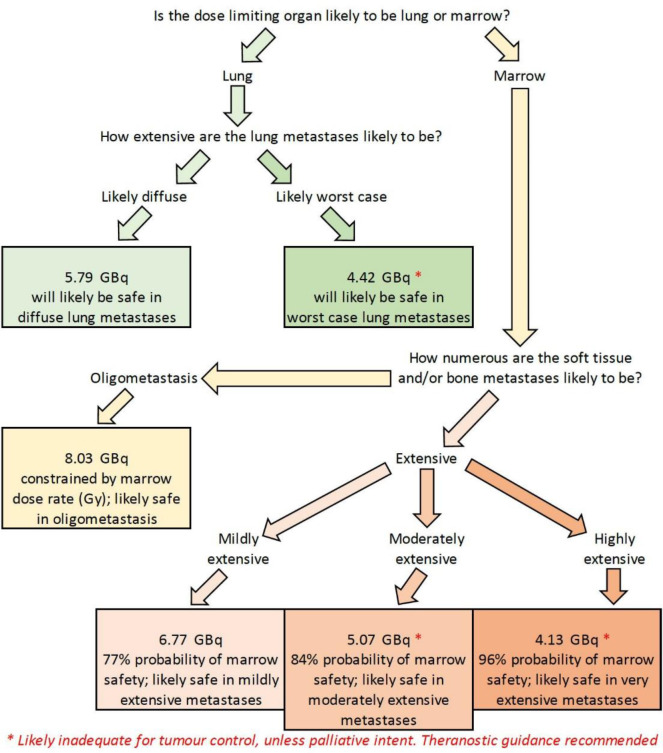
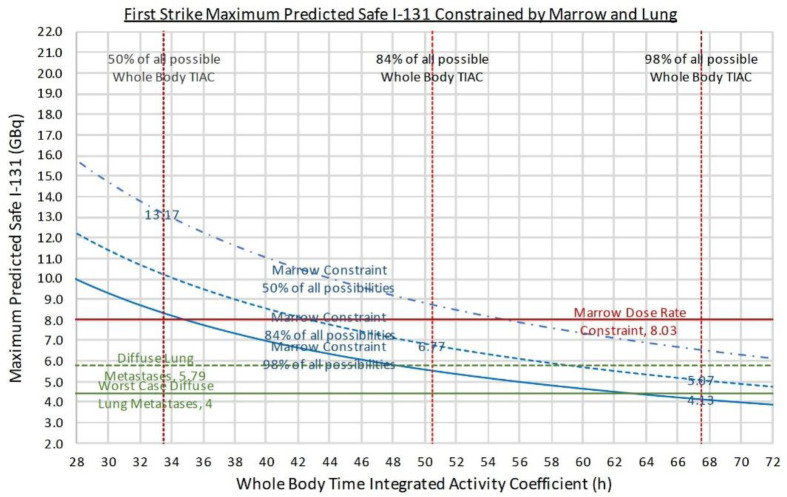
Results: The slowest whole body Time Integrated Activity Coefficient (TIAC) amongst patients with any metastases was 33.5±17.0 h and the highest percentage of whole body TIAC attributed to blood was 16.6±7.9%, prepared by thyroid hormone withdrawal. A variety of other average radioiodine kinetics is tabulated. Maximum safe marrow dose rate was deduced to be 0.265 Gy/h per fraction, where blood TIAC is normalised to administered activity. An easy-to-use calculator was developed which only requires height, weight and gender to populate recommendations for personalized First Strike prescription. The user decides by clinical gestalt whether the prescription is to be constrained by marrow or lung, then selects an activity depending on how extensive the metastases are likely to be. A Standard Female with oligometastasis and good urine output without diffuse lung metastasis is expected to safely tolerate 8.03 GBq of radioiodine as the First Strike.
Conclusion: This predictive method will help institutions rationalise the First Strike prescription based on radiobiologically sound principles, personalised to individual circumstances.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


