Alberto Palazzuoli MD, PhD, FESC , Alessandra Cartocci PhD , Filippo Pirrotta MD , Francesca Vannuccini MD , Alessandro Campora MD , Luca Martini MD , Frank Loyd Dini MD , Erberto Carluccio MD, FEACVI , Gaetano Ruocco MD
{"title":"左室射血分数对急性心力衰竭右室功能障碍和肺偶联的影响","authors":"Alberto Palazzuoli MD, PhD, FESC , Alessandra Cartocci PhD , Filippo Pirrotta MD , Francesca Vannuccini MD , Alessandro Campora MD , Luca Martini MD , Frank Loyd Dini MD , Erberto Carluccio MD, FEACVI , Gaetano Ruocco MD","doi":"10.1016/j.pcad.2023.07.008","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p><span>Right ventricular (RV) dysfunction and pulmonary uncoupling are two acknowledged features associated with poor outcome, however few data defined RV adaptation across the different left ventricular ejection fraction (EF) cut-off. Additionally, less data are reported </span>in patients<span> with acute heart failure (AHF).</span></p></div><div><h3>Aims</h3><p>The aim of present study was to analyse RV function<span> in AHF patients presenting with either reduced or preserved EF.</span></p></div><div><h3>Methods</h3><p>This is a multi-center observational study including 380 patients affected by AHF: 235 had AHF with reduced EF (AHFrEF) and 145 had AHF with preserved EF<span> (AHFpEF). Pulmonary artery systolic pressure<span> (PASP), tricuspid annular plane systolic excursion (TAPSE), S′ wave velocity, and the RV end-diastolic diameter (RVEDD) were measured by echocardiography. TAPSE/PASP and S′/PASP ratios were calculated as non-invasive surrogates of RV-pulmonary arterial coupling.</span></span></p></div><div><h3>Results</h3><p>Factors associated with poor outcome were higher values of PASP (45 [40–55] mmHg vs 40 [35–46] mmHg; <em>p</em> < 0.001), RVEDD (44 [38–47] mm vs 37 [35–42] mm; p < 0.001), lower TAPSE values (17 [15–20] mm vs 20 [18–22] mm; <em>p</em> < 0.001) and S′ wave (10 [8–12] cm/s vs 11 [10–13] cm/s; <em>p</em> < 0.001), reduced TAPSE/PASP (0.37 [0.29–0.47] vs 0.50 [0.40–0.60]; p < 0.001) and S′/PASP ratios (0.22 [0.18–0.28] vs 0.28 [0.22–0.34]; p < 0.001). However, the prognostic parameters differed according to the LVEF value: in AHFpEF S′/PASP between 0.22 and 0.29 and > 0.29 demonstrated a protective prognostic value (Respectively HR 0.29 (0.16–0.53), <em>p</em> < 0.001 and HR 0.22 [0.12–0.42], p < 0.001). Conversely, in AHFrEF, TAPSE <16 mm (HR 2.59 [1.67–4.03], p < 0.001), ICV > 21 mm (HR 1.17 [1.17–1.28], <em>p</em> = 0.001) and TAPSE/PASP <0.49 HR 1.92 [1.10–3.37], <em>p</em><span> = 0.023) were related to adverse outcome.</span></p></div><div><h3>Conclusions</h3><p>RV adaptation and RV pulmonary coupling differ in AHF according to the level of LVEF. S′ wave, and S′/PASP are associated with adverse outcome in patients with preserved EF; reduced TAPSE and TAPSE/PASP are better prognostic predictors in patients with reduced EF.</p></div>","PeriodicalId":21156,"journal":{"name":"Progress in cardiovascular diseases","volume":"81 ","pages":"Pages 89-97"},"PeriodicalIF":5.6000,"publicationDate":"2023-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Different right ventricular dysfunction and pulmonary coupling in acute heart failure according to the left ventricular ejection fraction\",\"authors\":\"Alberto Palazzuoli MD, PhD, FESC , Alessandra Cartocci PhD , Filippo Pirrotta MD , Francesca Vannuccini MD , Alessandro Campora MD , Luca Martini MD , Frank Loyd Dini MD , Erberto Carluccio MD, FEACVI , Gaetano Ruocco MD\",\"doi\":\"10.1016/j.pcad.2023.07.008\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p><span>Right ventricular (RV) dysfunction and pulmonary uncoupling are two acknowledged features associated with poor outcome, however few data defined RV adaptation across the different left ventricular ejection fraction (EF) cut-off. Additionally, less data are reported </span>in patients<span> with acute heart failure (AHF).</span></p></div><div><h3>Aims</h3><p>The aim of present study was to analyse RV function<span> in AHF patients presenting with either reduced or preserved EF.</span></p></div><div><h3>Methods</h3><p>This is a multi-center observational study including 380 patients affected by AHF: 235 had AHF with reduced EF (AHFrEF) and 145 had AHF with preserved EF<span> (AHFpEF). Pulmonary artery systolic pressure<span> (PASP), tricuspid annular plane systolic excursion (TAPSE), S′ wave velocity, and the RV end-diastolic diameter (RVEDD) were measured by echocardiography. TAPSE/PASP and S′/PASP ratios were calculated as non-invasive surrogates of RV-pulmonary arterial coupling.</span></span></p></div><div><h3>Results</h3><p>Factors associated with poor outcome were higher values of PASP (45 [40–55] mmHg vs 40 [35–46] mmHg; <em>p</em> < 0.001), RVEDD (44 [38–47] mm vs 37 [35–42] mm; p < 0.001), lower TAPSE values (17 [15–20] mm vs 20 [18–22] mm; <em>p</em> < 0.001) and S′ wave (10 [8–12] cm/s vs 11 [10–13] cm/s; <em>p</em> < 0.001), reduced TAPSE/PASP (0.37 [0.29–0.47] vs 0.50 [0.40–0.60]; p < 0.001) and S′/PASP ratios (0.22 [0.18–0.28] vs 0.28 [0.22–0.34]; p < 0.001). However, the prognostic parameters differed according to the LVEF value: in AHFpEF S′/PASP between 0.22 and 0.29 and > 0.29 demonstrated a protective prognostic value (Respectively HR 0.29 (0.16–0.53), <em>p</em> < 0.001 and HR 0.22 [0.12–0.42], p < 0.001). Conversely, in AHFrEF, TAPSE <16 mm (HR 2.59 [1.67–4.03], p < 0.001), ICV > 21 mm (HR 1.17 [1.17–1.28], <em>p</em> = 0.001) and TAPSE/PASP <0.49 HR 1.92 [1.10–3.37], <em>p</em><span> = 0.023) were related to adverse outcome.</span></p></div><div><h3>Conclusions</h3><p>RV adaptation and RV pulmonary coupling differ in AHF according to the level of LVEF. S′ wave, and S′/PASP are associated with adverse outcome in patients with preserved EF; reduced TAPSE and TAPSE/PASP are better prognostic predictors in patients with reduced EF.</p></div>\",\"PeriodicalId\":21156,\"journal\":{\"name\":\"Progress in cardiovascular diseases\",\"volume\":\"81 \",\"pages\":\"Pages 89-97\"},\"PeriodicalIF\":5.6000,\"publicationDate\":\"2023-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Progress in cardiovascular diseases\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0033062023000749\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Progress in cardiovascular diseases","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0033062023000749","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:右心室功能障碍和肺分离是两个公认的与预后不良相关的特征,然而很少有数据定义不同左心室射血分数(EF)截止值的右心室适应性。此外,关于急性心力衰竭(AHF)患者的数据报道较少。目的:本研究的目的是分析心室功能减少或保留的AHF患者的心室功能。方法:这是一项多中心观察性研究,包括380例AHF患者:235例AHF合并EF减缩(AHFrEF), 145例AHF合并EF保留(AHFpEF)。超声心动图测量肺动脉收缩压(PASP)、三尖瓣环形平面收缩偏移(TAPSE)、S波速度和右心室舒张末期内径(RVEDD)。计算TAPSE/PASP和S’/PASP比值作为rv -肺动脉耦合的无创替代指标。结果与预后不良相关的因素是PASP值较高(45 [40 - 55]mmHg vs 40 [35-46] mmHg;p & lt;0.001), RVEDD (44 [38-47] mm vs 37 [35-42] mm;p & lt;0.001),较低的TAPSE值(17 [15-20]mm vs 20 [18-22] mm;p & lt;0.001)和S波(10 [8-12]cm/ S vs 11 [10 - 13] cm/ S;p & lt;0.001),降低的TAPSE/PASP (0.37 [0.29-0.47] vs 0.50 [0.40-0.60];p & lt;0.001)和S ' /PASP比值(0.22 [0.18-0.28]vs 0.28 [0.22 - 0.34];p & lt;0.001)。然而,根据LVEF值,预后参数有所不同:AHFpEF S ' /PASP在0.22 - 0.29之间;0.29表现出预后保护价值(HR分别为0.29 (0.16-0.53),p <0.001和HR 0.22 [0.12-0.42], p <0.001)。相反,在AHFrEF中,TAPSE <16 mm (HR 2.59 [1.67-4.03], p <0.001), ICV >21 mm (HR 1.17 [1.17 - 1.28], p = 0.001)和TAPSE/PASP <0.49 HR 1.92 [1.10-3.37], p = 0.023)与不良结局相关。结论随着LVEF水平的不同,AHF的srv适应性和RV肺偶联存在差异。S '波和S ' /PASP与保留EF患者的不良预后相关;减少的TAPSE和TAPSE/PASP是EF减少患者更好的预后预测指标。
Different right ventricular dysfunction and pulmonary coupling in acute heart failure according to the left ventricular ejection fraction
Background
Right ventricular (RV) dysfunction and pulmonary uncoupling are two acknowledged features associated with poor outcome, however few data defined RV adaptation across the different left ventricular ejection fraction (EF) cut-off. Additionally, less data are reported in patients with acute heart failure (AHF).
Aims
The aim of present study was to analyse RV function in AHF patients presenting with either reduced or preserved EF.
Methods
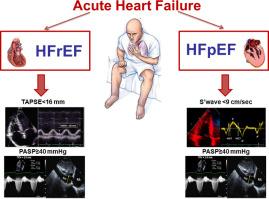
This is a multi-center observational study including 380 patients affected by AHF: 235 had AHF with reduced EF (AHFrEF) and 145 had AHF with preserved EF (AHFpEF). Pulmonary artery systolic pressure (PASP), tricuspid annular plane systolic excursion (TAPSE), S′ wave velocity, and the RV end-diastolic diameter (RVEDD) were measured by echocardiography. TAPSE/PASP and S′/PASP ratios were calculated as non-invasive surrogates of RV-pulmonary arterial coupling.
Results
Factors associated with poor outcome were higher values of PASP (45 [40–55] mmHg vs 40 [35–46] mmHg; p < 0.001), RVEDD (44 [38–47] mm vs 37 [35–42] mm; p < 0.001), lower TAPSE values (17 [15–20] mm vs 20 [18–22] mm; p < 0.001) and S′ wave (10 [8–12] cm/s vs 11 [10–13] cm/s; p < 0.001), reduced TAPSE/PASP (0.37 [0.29–0.47] vs 0.50 [0.40–0.60]; p < 0.001) and S′/PASP ratios (0.22 [0.18–0.28] vs 0.28 [0.22–0.34]; p < 0.001). However, the prognostic parameters differed according to the LVEF value: in AHFpEF S′/PASP between 0.22 and 0.29 and > 0.29 demonstrated a protective prognostic value (Respectively HR 0.29 (0.16–0.53), p < 0.001 and HR 0.22 [0.12–0.42], p < 0.001). Conversely, in AHFrEF, TAPSE <16 mm (HR 2.59 [1.67–4.03], p < 0.001), ICV > 21 mm (HR 1.17 [1.17–1.28], p = 0.001) and TAPSE/PASP <0.49 HR 1.92 [1.10–3.37], p = 0.023) were related to adverse outcome.
Conclusions
RV adaptation and RV pulmonary coupling differ in AHF according to the level of LVEF. S′ wave, and S′/PASP are associated with adverse outcome in patients with preserved EF; reduced TAPSE and TAPSE/PASP are better prognostic predictors in patients with reduced EF.
期刊介绍:
Progress in Cardiovascular Diseases provides comprehensive coverage of a single topic related to heart and circulatory disorders in each issue. Some issues include special articles, definitive reviews that capture the state of the art in the management of particular clinical problems in cardiology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


