Peter J. Abraham MD, MSPH, Rongzhi Wang MD, Deepti Bahl MD, Pradeep Bhambhvani MD, Sadie Ho, Jessica M. Fazendin MD, Herbert Chen MD, Brenessa M. Lindeman MD, MEHP
{"title":"Virtual Tumor Board: Papillary thyroid carcinoma with nodal disease","authors":"Peter J. Abraham MD, MSPH, Rongzhi Wang MD, Deepti Bahl MD, Pradeep Bhambhvani MD, Sadie Ho, Jessica M. Fazendin MD, Herbert Chen MD, Brenessa M. Lindeman MD, MEHP","doi":"10.3322/caac.21802","DOIUrl":null,"url":null,"abstract":"<p>The patient is a 19-year-old female who had an incidental thyroid nodule discovered on magnetic resonance imaging (MRI) in July 2020 during the work-up of a superficial, midline neck cellulitis. She reported having noticed a bulge in her neck a few years prior but had never been concerned about it. She began seeing an endocrinologist and underwent a thyroid ultrasound in July 2020, which revealed a solid, hypoechoic nodule in the left upper thyroid lobe measuring 2.2 cm in greatest dimension, classified as American College of Radiology Thyroid Imaging Reporting and Data System (ACR TI-RADS) 4 (Figure 1). Multiple, enlarged, abnormal-appearing lymph nodes were also noted in the left cervical lymph node chain in level IV (Figure 2). The lower pole of the left thyroid lobe was heterogeneous, with scattered calcifications and subcentimeter cystic areas, and no abnormal findings were noted in the isthmus or right lobe of the thyroid gland. Her thyroid function tests were normal, with a thyroid-stimulating hormone (TSH) level of 2.34 mU/L (reference range, 0.45–5.33 mU/L) and a T4 (thyroxine) level of 0.88 ng/dL (reference range, 0.58–1.64 μg/dL), with negative thyroid peroxidase antibodies and normal blood cell counts.</p><p>A fine-needle aspiration (FNA) of the left thyroid nodule was performed in September 2020 and revealed papillary thyroid cancer (PTC). The patient was then referred to the endocrine surgery clinic for evaluation and further management. An FNA biopsy of the concerning left lateral cervical lymph nodes (Figure 2) was conducted in the endocrine surgery clinic because it had not previously been performed. Given the concerning appearance of the lymph nodes on ultrasound, a total thyroidectomy with possible left central and lateral neck dissections was discussed as the likely operation pending pathology results from the lymph node biopsy. The patient agreed with the treatment plan, and FNA results from the lymph nodes returned as metastatic PTC.</p><p>Given the evidence of metastatic lymph node disease, the patient underwent a total thyroidectomy along with left central and lateral neck dissections in October 2020. Intraoperatively, a very firm nodule in the left lobe of the thyroid gland was encountered that was unable to be cleanly separated from the overlying sternothyroid muscle. Given concern for extrathyroidal extension, the muscle was resected en bloc with the thyroid specimen. During the dissection, there was concern for devascularization of the left superior parathyroid gland, so it was excised and re-implanted. However, there was significant lymphadenopathy low in cervical level VI surrounding the left inferior parathyroid gland, making clear identification of the inferior gland difficult. A frozen section was obtained that confirmed the identification of the left inferior parathyroid gland, so it was also re-implanted into the left sternocleidomastoid muscle. Bulky lymphadenopathy was found throughout the left central and lateral neck (levels II–VI) during the neck dissection.</p><p>Surgical pathology revealed a greatest tumor dimension of 4.5 cm with lymphovascular invasion but no extrathyroidal extension and clear resection margins. Five of the seven resected lymph nodes from the central neck and nine of the 19 nodes in the lateral neck showed PTC without extranodal extension. The overall pathologic stage was pT3aN1b.</p><p>Postoperatively, the patient experienced transient hypocalcemia, which required 8 weeks of calcium supplementation. Her 6-week postoperative thyroglobulin (Tg) level was 0.6 ng/mL in December 2020. A diagnostic whole-body scan in January 2021 revealed physiologic uptake in the thyroidectomy bed with no evidence of metastatic disease. She subsequently underwent radioactive iodine (RAI) therapy with 157.7 millicuries (mCi) of iodine-131 (<sup>131</sup>I), and her postablation scan similarly showed physiologic uptake in the thyroidectomy bed with no evidence of metastatic disease (Figures 3 and 4). Subsequent thyroid ultrasound studies in April and September of 2021 also showed no evidence of recurrent disease or suspicious findings throughout the thyroid bed or bilateral cervical chains I–VI. Her Tg level was undetectable (<0.1 ng/mL) in October 2021 after her RAI therapy.</p><p>At presentation, this is a young female with an incidentally diagnosed thyroid nodule. The initial evaluation for thyroid nodule(s) is comprised of a thorough history and physical examination, including evaluation for symptoms of hypothyroidism or hyperthyroidism. Pertinent history that increases the risk of malignancy includes a history of head or neck radiation, patient extremes of age (younger than 14 or older than 70 years), history of rapid growth of the nodule(s), persistent dysphonia, male gender,<span><sup>1</sup></span> and significant family history of differentiated thyroid cancer, medullary thyroid cancer, or multiple endocrine neoplasia type 2.</p><p>The initial laboratory work-up to evaluate a thyroid nodule includes a TSH level. A suppressed or low TSH level, which signifies a hyperthyroid state, is associated with a decreased probability of malignancy (approximately 3%).<span><sup>2, 3</sup></span> Conversely, an increased level of serum TSH, even when the level is still within reference limits, is statistically associated with an increased risk of cancer in thyroid nodular disease.<span><sup>4</sup></span></p><p>A diagnostic thyroid ultrasound with evaluation of cervical lymph nodes is recommended for all patients with a known or suspected thyroid nodule.<span><sup>5</sup></span> FNA is the procedure of choice for the histologic evaluation of thyroid nodules. The nodule size at initial ultrasound; the ultrasound characteristics, which include the composition (solid vs. cystic), echogenicity, shape, and margins of the nodule; and an increase in size during follow-up determine the need for FNA.<span><sup>6, 7</sup></span> FNA is typically performed under ultrasound guidance to ensure optimal placement of the needle. In the United States, the two commonly used guidelines to estimate risk of malignancy and thus assess a need for FNA are the American Thyroid Association (ATA) guidelines<span><sup>8</sup></span> and the ACR TI-RADS.<span><sup>6, 9</sup></span> Both guidelines recommend biopsy if the thyroid nodule has high-suspicion sonographic features and is over a specific size threshold.<span><sup>10</sup></span> In this patient, an FNA was indicated given her euthyroid state (normal TSH), her enlarged nodule size (>1 cm), concerning features on ultrasound (solid, hypoechoic), as well as the presence of abnormal-appearing lymph nodes in the left cervical lymph node chain level IV.<span><sup>11</sup></span></p><p>Adjuvant therapy for thyroid cancer in the form of RAI is considered when patients have a higher risk of persistent or recurrent disease after surgical intervention.<span><sup>12</sup></span> According to ATA guidelines, patients with gross extrathyroidal extension, incomplete tumor resection, lymph node metastasis >3 cm, the presence of extranodal extension, or distant metastases are deemed high-risk (30%–50% risk of recurrence) and are routinely considered for RAI. In addition, patients with aggressive histology, minor extrathyroidal extension, vascular invasion, or greater than five lymph node metastases in the central or lateral cervical compartments are considered intermediate-risk (10%–30% risk of recurrence) and are generally favored for RAI therapy.<span><sup>8</sup></span> Intrathyroidal differentiated thyroid cancer with five or fewer lymph node micrometastases is generally considered low-risk (<5%–10% risk of recurrence), and RAI therapy is not recommended in these patients. Postoperative serum Tg can help in assessing the persistence of disease or thyroid remnant and predicting potential future disease recurrence. The Tg level reaches its nadir by 3–4 weeks postoperatively in most patients. At our institution, we routinely check the Tg level 4–6 weeks postoperatively as a surveillance marker and to guide further adjuvant therapy. The patient's tumor size, the presence of lymphovascular invasion, and the involvement of greater than five lymph nodes in the neck (<3 cm in size) placed her in the intermediate-risk category, so RAI therapy was recommended to reduce her risk of persistent or recurrent disease.</p><p>Obtaining an adequate assessment of the lymph node-bearing compartments in the central and lateral neck is essential to performing a sufficient thyroid operation. Lymph nodes that appear abnormal on cervical ultrasound need to be biopsied because the presence of lymph node metastases will affect the extent of surgical resection required, as it has been demonstrated that intraoperative frozen-section analysis of the thyroid gland is unreliable and thus should not be routinely performed.<span><sup>13</sup></span> When the patient was first seen in the endocrine surgery clinic, biopsy of the concerning lymph nodes had not yet been completed, thus an FNA was performed during the initial endocrine surgery visit. To expedite care while awaiting the FNA pathology results, all operative possibilities were discussed with the patient during the initial visit, including lobectomy and total thyroidectomy with possible central and lateral neck dissections. Consent for the operation was obtained in the clinic, and the extent of the operation was confirmed by telephone after release of the FNA pathology result 1 week later. This expedited process allowed the patient to undergo her definitive operation, which was performed within 2 weeks of her initial surgical evaluation.</p><p>Although the presence of lymph node metastases was the primary driver for the decision to perform a total thyroidectomy, there were additional benefits, including the ability to perform postoperative RAI therapy and allowing for postoperative surveillance using the Tg level. These secondary benefits of removing the entire thyroid gland aided the multidisciplinary approach to the patient's care and allowed our nuclear medicine and endocrinology colleagues to provide additional therapy and closer monitoring.</p><p>At our institution, we often perform outpatient neck dissections and do not routinely leave a cervical drain.<span><sup>14</sup></span> Our outpatient thyroidectomy patients have a parathyroid hormone (PTH) level drawn once they arrive at the postoperative anesthesia care unit (PACU) and are monitored postoperatively in the PACU for 2–4 hours before discharge. We have a protocol that specifies the doses of calcium and calcitriol with which to send patients home based on the PACU PTH level, which considers high-risk features, such as the presence of hyperthyroidism. Patients then follow-up in the clinic in 1–2 weeks with calcium and PTH levels drawn at that time. All total thyroidectomy patients are started on levothyroxine postoperatively with TSH and Tg levels drawn at 6 weeks postoperatively.</p><p>Multiple studies have demonstrated the safety of performing outpatient total thyroidectomy,<span><sup>14-17</sup></span> and it has become an increasingly common practice among endocrine surgeons. Additional studies have demonstrated no difference in the complication rate when central and/or lateral neck dissections are concurrently performed with the total thyroidectomy, and increasing numbers of endocrine surgeons safely perform these operations on an outpatient basis.<span><sup>18-20</sup></span> Similarly, studies have indicated that the placement of a drain does not reduce the risk of hematoma formation or other complications, including chyle leak, in post-thyroidectomy patients,<span><sup>21, 22</sup></span> even after lateral neck dissection.<span><sup>23-26</sup></span> Given our patient's lack of other comorbidities, any predisposing risk factor for a hematoma, or gross evidence of chyle leak intraoperatively, an outpatient operation without drain placement was chosen and successfully performed without complication.</p><p>The decision between a selective and modified radical neck dissection was another important one to consider in this patient. Some evidence suggests that a compartment-oriented lymphadenectomy is all that is needed for macroscopic nodal disease and that no benefit is gained by adding a complete level V dissection unless there is evidence of metastasis in level V or extensive (three-compartment) disease.<span><sup>27, 28</sup></span> Our patient's nodal disease appeared to be limited to cervical levels III and IV, so she underwent a selective neck dissection of the lateral neck involving compartments II–IV with a partial level V dissection. This compartment-oriented dissection was performed to balance the removal of all macroscopic nodal disease with the attempt to minimize morbidity associated with radical neck dissections.</p><p>Radioiodine (<sup>131</sup>I) therapy has been used in the management of patients with well differentiated PTC or follicular thyroid cancer since the 1940s for remnant ablation and as adjuvant treatment for subclinical, residual tumor or for macroscopic, metastatic disease. Treatment benefits include enabling disease monitoring with serum Tg and radioiodine scans; and, in intermediate-risk and high-risk patients, there are added benefits of a decreased risk of recurrence and improved disease-specific, progression-free, and overall survival. The thyroid follicular cell has a unique ability to take up iodine from the blood through its membrane sodium-iodide transporter. After uptake by this active transport process, <sup>131</sup>I causes acute thyroid cell death by the emission of short path-length (1–2 mm) beta particles. The identification and localization of uptake foci may be enhanced by a concomitant single-photon emission computed tomography/computed tomography (SPECT/CT) scan.<span><sup>8</sup></span> Diagnostic whole-body scans (WBS) are acquired 1–3 days after RAI administration, whereas post-RAI treatment images can be obtained 2–7 days after treatment.<span><sup>29</sup></span></p><p>The routine use of a preablation or diagnostic WBS with SPECT/CT is controversial, and there continues to be discussion on the utility of postoperative RAI diagnostic scanning (with or without SPECT/CT) in guiding RAI therapeutic decision making. According to the ATA, WBS may be useful when the extent of the thyroid remnant or residual disease cannot be accurately ascertained from the surgical report or neck ultrasonography and when the results may alter the decision to treat or the activity of RAI that is to be administered. For example, scan findings could suggest the need for additional surgery for resectable residual tumor or possibly could increase the administered activity if there is identification of otherwise unknown metastatic disease. Cons of WBS include the potential for stunning the thyroid follicular cells by the low dose of radioiodine used, which may lower uptake of the subsequent therapeutic radioiodine.<span><sup>30</sup></span> In addition, it is well documented that a diagnostic, low-dose RAI scan is frequently falsely negative, but the post-<sup>131</sup>I therapy scan is positive for functioning <sup>131</sup>I-avid metastases.<span><sup>12</sup></span></p><p>Based on age-based TNM staging, the patient had stage I disease, but the ATA risk-stratification system put our patient at intermediate risk of persistent/recurrent disease because she had greater than five enlarged lateral neck nodes measuring ≤3 cm in greatest dimension.<span><sup>8, 31</sup></span> For the treatment of thyroid cancer involving cervical lymph nodes, <sup>131</sup>I activity in the range from 5.55 to 7.4 gigabecquerels (150–200 mCi) is typically administered to adults.<span><sup>30</sup></span> According to ATA recommendations for adjuvant RAI therapy for suspected microscopic residual disease, it is uncertain whether routine use of higher administered activities (>150 mCi) will reduce structural disease recurrence for T3 and N1 disease.<span><sup>8</sup></span> Therefore, <sup>131</sup>I activity of approximately 150 mCi was selected for our patient. Figure 3 shows the posttherapy WBS with physiologic uptake in the thyroid bed and absence of radioiodine-avid nodal or distant metastatic disease. The small focus to the right of thyroid bed activity on the WBS (Figure 3, arrow) is artifactual from patient motion because the same is not seen on the static head and neck images (Figure 4).</p><p>As discussed above, nuclear medicine physicians are divided about the need for postoperative diagnostic low-activity radioiodine (1–3 mCi; <sup>131</sup>I or <sup>123</sup>I) WBS.<span><sup>29</sup></span> If there were no remnants or other foci of iodine-avid tissue on the scan, then giving radioiodine would not be indicated; however, in high-risk patients, RAI treatment of occult metastases may be warranted.<span><sup>29</sup></span> In our patient, the diagnostic scan was performed given the risk factors of muscle invasion and multiple nodal metastases. If additional resectable disease had been identified on the preablation scan, then referral to surgery would have been a reasonable consideration. Alternatively, if she had distant tumor spread (e.g. lung or bone) identified, then the administered radioiodine activity would have been increased. In her case, neither both the pretherapy and posttherapy scans did not identify additional resectable tumor or metastatic disease, and thus the treatment plan or <sup>131</sup>I activity (150 mCi) was not altered.</p><p>PTC with nodal metastases is a complex disease that requires a multidisciplinary team approach. Adequate treatment of the disease requires the careful integration of multiple medical services, including endocrinology, endocrine surgery, and nuclear medicine. Clear communication between the various teams and the patient is essential to keeping the patient well informed and maintaining patient autonomy. Ultimately, a multidisciplinary approach can provide excellent care for patients with thyroid cancer and especially should be pursued in instances of lymph node metastases.</p><p>The authors declared no conflicts of interest.</p>","PeriodicalId":137,"journal":{"name":"CA: A Cancer Journal for Clinicians","volume":"73 6","pages":"555-561"},"PeriodicalIF":503.1000,"publicationDate":"2023-06-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CA: A Cancer Journal for Clinicians","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.3322/caac.21802","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
The patient is a 19-year-old female who had an incidental thyroid nodule discovered on magnetic resonance imaging (MRI) in July 2020 during the work-up of a superficial, midline neck cellulitis. She reported having noticed a bulge in her neck a few years prior but had never been concerned about it. She began seeing an endocrinologist and underwent a thyroid ultrasound in July 2020, which revealed a solid, hypoechoic nodule in the left upper thyroid lobe measuring 2.2 cm in greatest dimension, classified as American College of Radiology Thyroid Imaging Reporting and Data System (ACR TI-RADS) 4 (Figure 1). Multiple, enlarged, abnormal-appearing lymph nodes were also noted in the left cervical lymph node chain in level IV (Figure 2). The lower pole of the left thyroid lobe was heterogeneous, with scattered calcifications and subcentimeter cystic areas, and no abnormal findings were noted in the isthmus or right lobe of the thyroid gland. Her thyroid function tests were normal, with a thyroid-stimulating hormone (TSH) level of 2.34 mU/L (reference range, 0.45–5.33 mU/L) and a T4 (thyroxine) level of 0.88 ng/dL (reference range, 0.58–1.64 μg/dL), with negative thyroid peroxidase antibodies and normal blood cell counts.
A fine-needle aspiration (FNA) of the left thyroid nodule was performed in September 2020 and revealed papillary thyroid cancer (PTC). The patient was then referred to the endocrine surgery clinic for evaluation and further management. An FNA biopsy of the concerning left lateral cervical lymph nodes (Figure 2) was conducted in the endocrine surgery clinic because it had not previously been performed. Given the concerning appearance of the lymph nodes on ultrasound, a total thyroidectomy with possible left central and lateral neck dissections was discussed as the likely operation pending pathology results from the lymph node biopsy. The patient agreed with the treatment plan, and FNA results from the lymph nodes returned as metastatic PTC.
Given the evidence of metastatic lymph node disease, the patient underwent a total thyroidectomy along with left central and lateral neck dissections in October 2020. Intraoperatively, a very firm nodule in the left lobe of the thyroid gland was encountered that was unable to be cleanly separated from the overlying sternothyroid muscle. Given concern for extrathyroidal extension, the muscle was resected en bloc with the thyroid specimen. During the dissection, there was concern for devascularization of the left superior parathyroid gland, so it was excised and re-implanted. However, there was significant lymphadenopathy low in cervical level VI surrounding the left inferior parathyroid gland, making clear identification of the inferior gland difficult. A frozen section was obtained that confirmed the identification of the left inferior parathyroid gland, so it was also re-implanted into the left sternocleidomastoid muscle. Bulky lymphadenopathy was found throughout the left central and lateral neck (levels II–VI) during the neck dissection.
Surgical pathology revealed a greatest tumor dimension of 4.5 cm with lymphovascular invasion but no extrathyroidal extension and clear resection margins. Five of the seven resected lymph nodes from the central neck and nine of the 19 nodes in the lateral neck showed PTC without extranodal extension. The overall pathologic stage was pT3aN1b.
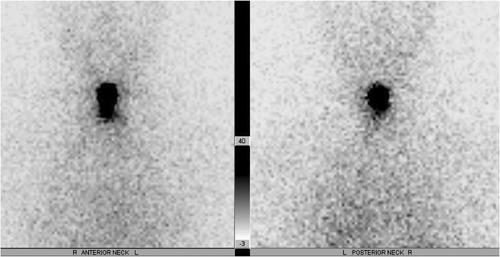
Postoperatively, the patient experienced transient hypocalcemia, which required 8 weeks of calcium supplementation. Her 6-week postoperative thyroglobulin (Tg) level was 0.6 ng/mL in December 2020. A diagnostic whole-body scan in January 2021 revealed physiologic uptake in the thyroidectomy bed with no evidence of metastatic disease. She subsequently underwent radioactive iodine (RAI) therapy with 157.7 millicuries (mCi) of iodine-131 (131I), and her postablation scan similarly showed physiologic uptake in the thyroidectomy bed with no evidence of metastatic disease (Figures 3 and 4). Subsequent thyroid ultrasound studies in April and September of 2021 also showed no evidence of recurrent disease or suspicious findings throughout the thyroid bed or bilateral cervical chains I–VI. Her Tg level was undetectable (<0.1 ng/mL) in October 2021 after her RAI therapy.
At presentation, this is a young female with an incidentally diagnosed thyroid nodule. The initial evaluation for thyroid nodule(s) is comprised of a thorough history and physical examination, including evaluation for symptoms of hypothyroidism or hyperthyroidism. Pertinent history that increases the risk of malignancy includes a history of head or neck radiation, patient extremes of age (younger than 14 or older than 70 years), history of rapid growth of the nodule(s), persistent dysphonia, male gender,1 and significant family history of differentiated thyroid cancer, medullary thyroid cancer, or multiple endocrine neoplasia type 2.
The initial laboratory work-up to evaluate a thyroid nodule includes a TSH level. A suppressed or low TSH level, which signifies a hyperthyroid state, is associated with a decreased probability of malignancy (approximately 3%).2, 3 Conversely, an increased level of serum TSH, even when the level is still within reference limits, is statistically associated with an increased risk of cancer in thyroid nodular disease.4
A diagnostic thyroid ultrasound with evaluation of cervical lymph nodes is recommended for all patients with a known or suspected thyroid nodule.5 FNA is the procedure of choice for the histologic evaluation of thyroid nodules. The nodule size at initial ultrasound; the ultrasound characteristics, which include the composition (solid vs. cystic), echogenicity, shape, and margins of the nodule; and an increase in size during follow-up determine the need for FNA.6, 7 FNA is typically performed under ultrasound guidance to ensure optimal placement of the needle. In the United States, the two commonly used guidelines to estimate risk of malignancy and thus assess a need for FNA are the American Thyroid Association (ATA) guidelines8 and the ACR TI-RADS.6, 9 Both guidelines recommend biopsy if the thyroid nodule has high-suspicion sonographic features and is over a specific size threshold.10 In this patient, an FNA was indicated given her euthyroid state (normal TSH), her enlarged nodule size (>1 cm), concerning features on ultrasound (solid, hypoechoic), as well as the presence of abnormal-appearing lymph nodes in the left cervical lymph node chain level IV.11
Adjuvant therapy for thyroid cancer in the form of RAI is considered when patients have a higher risk of persistent or recurrent disease after surgical intervention.12 According to ATA guidelines, patients with gross extrathyroidal extension, incomplete tumor resection, lymph node metastasis >3 cm, the presence of extranodal extension, or distant metastases are deemed high-risk (30%–50% risk of recurrence) and are routinely considered for RAI. In addition, patients with aggressive histology, minor extrathyroidal extension, vascular invasion, or greater than five lymph node metastases in the central or lateral cervical compartments are considered intermediate-risk (10%–30% risk of recurrence) and are generally favored for RAI therapy.8 Intrathyroidal differentiated thyroid cancer with five or fewer lymph node micrometastases is generally considered low-risk (<5%–10% risk of recurrence), and RAI therapy is not recommended in these patients. Postoperative serum Tg can help in assessing the persistence of disease or thyroid remnant and predicting potential future disease recurrence. The Tg level reaches its nadir by 3–4 weeks postoperatively in most patients. At our institution, we routinely check the Tg level 4–6 weeks postoperatively as a surveillance marker and to guide further adjuvant therapy. The patient's tumor size, the presence of lymphovascular invasion, and the involvement of greater than five lymph nodes in the neck (<3 cm in size) placed her in the intermediate-risk category, so RAI therapy was recommended to reduce her risk of persistent or recurrent disease.
Obtaining an adequate assessment of the lymph node-bearing compartments in the central and lateral neck is essential to performing a sufficient thyroid operation. Lymph nodes that appear abnormal on cervical ultrasound need to be biopsied because the presence of lymph node metastases will affect the extent of surgical resection required, as it has been demonstrated that intraoperative frozen-section analysis of the thyroid gland is unreliable and thus should not be routinely performed.13 When the patient was first seen in the endocrine surgery clinic, biopsy of the concerning lymph nodes had not yet been completed, thus an FNA was performed during the initial endocrine surgery visit. To expedite care while awaiting the FNA pathology results, all operative possibilities were discussed with the patient during the initial visit, including lobectomy and total thyroidectomy with possible central and lateral neck dissections. Consent for the operation was obtained in the clinic, and the extent of the operation was confirmed by telephone after release of the FNA pathology result 1 week later. This expedited process allowed the patient to undergo her definitive operation, which was performed within 2 weeks of her initial surgical evaluation.
Although the presence of lymph node metastases was the primary driver for the decision to perform a total thyroidectomy, there were additional benefits, including the ability to perform postoperative RAI therapy and allowing for postoperative surveillance using the Tg level. These secondary benefits of removing the entire thyroid gland aided the multidisciplinary approach to the patient's care and allowed our nuclear medicine and endocrinology colleagues to provide additional therapy and closer monitoring.
At our institution, we often perform outpatient neck dissections and do not routinely leave a cervical drain.14 Our outpatient thyroidectomy patients have a parathyroid hormone (PTH) level drawn once they arrive at the postoperative anesthesia care unit (PACU) and are monitored postoperatively in the PACU for 2–4 hours before discharge. We have a protocol that specifies the doses of calcium and calcitriol with which to send patients home based on the PACU PTH level, which considers high-risk features, such as the presence of hyperthyroidism. Patients then follow-up in the clinic in 1–2 weeks with calcium and PTH levels drawn at that time. All total thyroidectomy patients are started on levothyroxine postoperatively with TSH and Tg levels drawn at 6 weeks postoperatively.
Multiple studies have demonstrated the safety of performing outpatient total thyroidectomy,14-17 and it has become an increasingly common practice among endocrine surgeons. Additional studies have demonstrated no difference in the complication rate when central and/or lateral neck dissections are concurrently performed with the total thyroidectomy, and increasing numbers of endocrine surgeons safely perform these operations on an outpatient basis.18-20 Similarly, studies have indicated that the placement of a drain does not reduce the risk of hematoma formation or other complications, including chyle leak, in post-thyroidectomy patients,21, 22 even after lateral neck dissection.23-26 Given our patient's lack of other comorbidities, any predisposing risk factor for a hematoma, or gross evidence of chyle leak intraoperatively, an outpatient operation without drain placement was chosen and successfully performed without complication.
The decision between a selective and modified radical neck dissection was another important one to consider in this patient. Some evidence suggests that a compartment-oriented lymphadenectomy is all that is needed for macroscopic nodal disease and that no benefit is gained by adding a complete level V dissection unless there is evidence of metastasis in level V or extensive (three-compartment) disease.27, 28 Our patient's nodal disease appeared to be limited to cervical levels III and IV, so she underwent a selective neck dissection of the lateral neck involving compartments II–IV with a partial level V dissection. This compartment-oriented dissection was performed to balance the removal of all macroscopic nodal disease with the attempt to minimize morbidity associated with radical neck dissections.
Radioiodine (131I) therapy has been used in the management of patients with well differentiated PTC or follicular thyroid cancer since the 1940s for remnant ablation and as adjuvant treatment for subclinical, residual tumor or for macroscopic, metastatic disease. Treatment benefits include enabling disease monitoring with serum Tg and radioiodine scans; and, in intermediate-risk and high-risk patients, there are added benefits of a decreased risk of recurrence and improved disease-specific, progression-free, and overall survival. The thyroid follicular cell has a unique ability to take up iodine from the blood through its membrane sodium-iodide transporter. After uptake by this active transport process, 131I causes acute thyroid cell death by the emission of short path-length (1–2 mm) beta particles. The identification and localization of uptake foci may be enhanced by a concomitant single-photon emission computed tomography/computed tomography (SPECT/CT) scan.8 Diagnostic whole-body scans (WBS) are acquired 1–3 days after RAI administration, whereas post-RAI treatment images can be obtained 2–7 days after treatment.29
The routine use of a preablation or diagnostic WBS with SPECT/CT is controversial, and there continues to be discussion on the utility of postoperative RAI diagnostic scanning (with or without SPECT/CT) in guiding RAI therapeutic decision making. According to the ATA, WBS may be useful when the extent of the thyroid remnant or residual disease cannot be accurately ascertained from the surgical report or neck ultrasonography and when the results may alter the decision to treat or the activity of RAI that is to be administered. For example, scan findings could suggest the need for additional surgery for resectable residual tumor or possibly could increase the administered activity if there is identification of otherwise unknown metastatic disease. Cons of WBS include the potential for stunning the thyroid follicular cells by the low dose of radioiodine used, which may lower uptake of the subsequent therapeutic radioiodine.30 In addition, it is well documented that a diagnostic, low-dose RAI scan is frequently falsely negative, but the post-131I therapy scan is positive for functioning 131I-avid metastases.12
Based on age-based TNM staging, the patient had stage I disease, but the ATA risk-stratification system put our patient at intermediate risk of persistent/recurrent disease because she had greater than five enlarged lateral neck nodes measuring ≤3 cm in greatest dimension.8, 31 For the treatment of thyroid cancer involving cervical lymph nodes, 131I activity in the range from 5.55 to 7.4 gigabecquerels (150–200 mCi) is typically administered to adults.30 According to ATA recommendations for adjuvant RAI therapy for suspected microscopic residual disease, it is uncertain whether routine use of higher administered activities (>150 mCi) will reduce structural disease recurrence for T3 and N1 disease.8 Therefore, 131I activity of approximately 150 mCi was selected for our patient. Figure 3 shows the posttherapy WBS with physiologic uptake in the thyroid bed and absence of radioiodine-avid nodal or distant metastatic disease. The small focus to the right of thyroid bed activity on the WBS (Figure 3, arrow) is artifactual from patient motion because the same is not seen on the static head and neck images (Figure 4).
As discussed above, nuclear medicine physicians are divided about the need for postoperative diagnostic low-activity radioiodine (1–3 mCi; 131I or 123I) WBS.29 If there were no remnants or other foci of iodine-avid tissue on the scan, then giving radioiodine would not be indicated; however, in high-risk patients, RAI treatment of occult metastases may be warranted.29 In our patient, the diagnostic scan was performed given the risk factors of muscle invasion and multiple nodal metastases. If additional resectable disease had been identified on the preablation scan, then referral to surgery would have been a reasonable consideration. Alternatively, if she had distant tumor spread (e.g. lung or bone) identified, then the administered radioiodine activity would have been increased. In her case, neither both the pretherapy and posttherapy scans did not identify additional resectable tumor or metastatic disease, and thus the treatment plan or 131I activity (150 mCi) was not altered.
PTC with nodal metastases is a complex disease that requires a multidisciplinary team approach. Adequate treatment of the disease requires the careful integration of multiple medical services, including endocrinology, endocrine surgery, and nuclear medicine. Clear communication between the various teams and the patient is essential to keeping the patient well informed and maintaining patient autonomy. Ultimately, a multidisciplinary approach can provide excellent care for patients with thyroid cancer and especially should be pursued in instances of lymph node metastases.
期刊介绍:
CA: A Cancer Journal for Clinicians" has been published by the American Cancer Society since 1950, making it one of the oldest peer-reviewed journals in oncology. It maintains the highest impact factor among all ISI-ranked journals. The journal effectively reaches a broad and diverse audience of health professionals, offering a unique platform to disseminate information on cancer prevention, early detection, various treatment modalities, palliative care, advocacy matters, quality-of-life topics, and more. As the premier journal of the American Cancer Society, it publishes mission-driven content that significantly influences patient care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


