Ru Li, Tingyu Wang, Rui Lyv, Yi Wang, Ying Yu, Yuting Yan, Qi Sun, Wenjie Xiong, Wei Liu, Weiwei Sui, Wenyang Huang, Huijun Wang, Chengwen Li, Jun Wang, Dehui Zou, Gang An, Jianxiang Wang, Lugui Qiu, Shuhua Yi
{"title":"Benefit of rituximab maintenance is associated with Follicular Lymphoma International Prognostic Index in patients with follicular lymphoma.","authors":"Ru Li, Tingyu Wang, Rui Lyv, Yi Wang, Ying Yu, Yuting Yan, Qi Sun, Wenjie Xiong, Wei Liu, Weiwei Sui, Wenyang Huang, Huijun Wang, Chengwen Li, Jun Wang, Dehui Zou, Gang An, Jianxiang Wang, Lugui Qiu, Shuhua Yi","doi":"10.1097/BS9.0000000000000144","DOIUrl":null,"url":null,"abstract":"<p><p>Rituximab maintenance (RM) prolongs the progression-free survival (PFS) of responding patients with follicular lymphoma (FL), but the maintenance efficacy in different Follicular Lymphoma International Prognostic Index (FLIPI) risk group is still confusing. We performed a retrospective analysis of the effect of RM treatments in patients with FL responding to induction therapy based on their FLIPI risk assessment carried out prior to treatment. We identified 93 patients between 2013 and 2019 who received RM every 3 months for ≥4 doses (RM group), and 60 patients who did not accept RM or received rituximab less than 4 doses (control group). After a median follow-up of 39 months, neither median overall survival (OS) nor PFS was reached for the entire population. The PFS was significantly prolonged in the RM group compared to the control group (median PFS NA vs 83.1 months, <i>P</i> = .00027). When the population was divided into the 3 FLIPI risk groups, the PFS differed significantly (4-year PFS rates, 97.5% vs 88.8% vs 72.3%, <i>P</i> = .01) according to group. There was no significant difference in PFS for FLIPI low-risk patients with RM compared to the control group (4-year PFS rates, 100% vs 93.8%, <i>P</i> = .23). However, the PFS of the RM group was significantly prolonged for FLIPI intermediate-risk (4-year PFS rates, 100% vs 70.3%, <i>P</i> = .00077) and high-risk patients (4-year PFS rates, 86.7% vs 57.1%, <i>P</i> = .023). These data suggest that standard RM significantly prolongs the PFS of patients assigned to intermediate- and high-risk FLIPI groups but not to low-risk FLIPI group, and pending larger-scale studies to validate.</p>","PeriodicalId":67343,"journal":{"name":"血液科学(英文)","volume":"5 2","pages":"118-124"},"PeriodicalIF":1.5000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10205248/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"血液科学(英文)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/BS9.0000000000000144","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
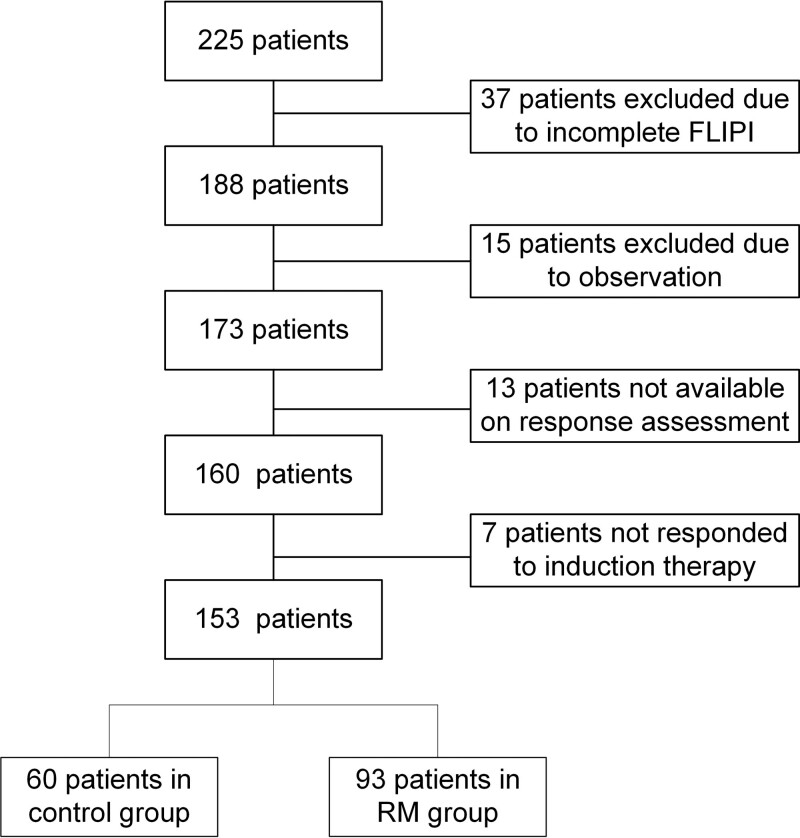
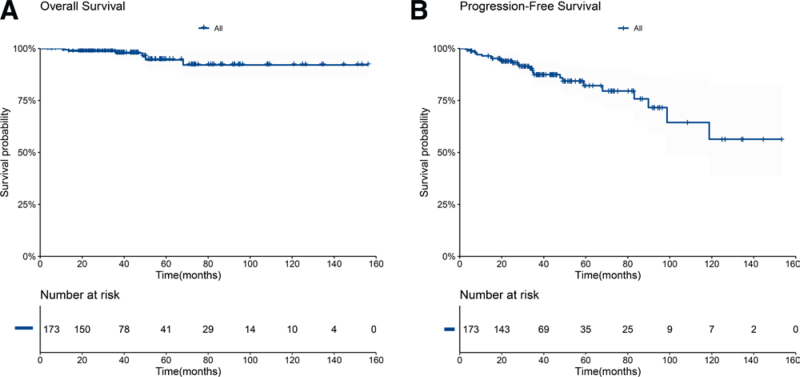
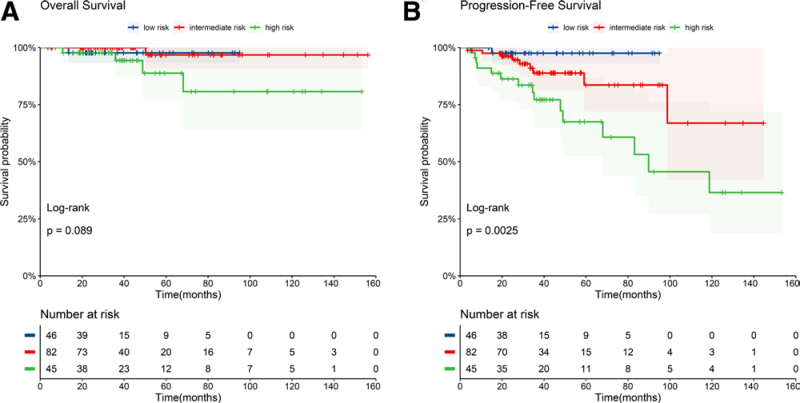
Rituximab maintenance (RM) prolongs the progression-free survival (PFS) of responding patients with follicular lymphoma (FL), but the maintenance efficacy in different Follicular Lymphoma International Prognostic Index (FLIPI) risk group is still confusing. We performed a retrospective analysis of the effect of RM treatments in patients with FL responding to induction therapy based on their FLIPI risk assessment carried out prior to treatment. We identified 93 patients between 2013 and 2019 who received RM every 3 months for ≥4 doses (RM group), and 60 patients who did not accept RM or received rituximab less than 4 doses (control group). After a median follow-up of 39 months, neither median overall survival (OS) nor PFS was reached for the entire population. The PFS was significantly prolonged in the RM group compared to the control group (median PFS NA vs 83.1 months, P = .00027). When the population was divided into the 3 FLIPI risk groups, the PFS differed significantly (4-year PFS rates, 97.5% vs 88.8% vs 72.3%, P = .01) according to group. There was no significant difference in PFS for FLIPI low-risk patients with RM compared to the control group (4-year PFS rates, 100% vs 93.8%, P = .23). However, the PFS of the RM group was significantly prolonged for FLIPI intermediate-risk (4-year PFS rates, 100% vs 70.3%, P = .00077) and high-risk patients (4-year PFS rates, 86.7% vs 57.1%, P = .023). These data suggest that standard RM significantly prolongs the PFS of patients assigned to intermediate- and high-risk FLIPI groups but not to low-risk FLIPI group, and pending larger-scale studies to validate.
利妥昔单抗维持治疗(RM)可延长滤泡性淋巴瘤(FL)患者的无进展生存期(PFS),但不同滤泡性淋巴瘤国际预后指数(FLIPI)风险组的维持疗效尚不明确。我们基于治疗前对FL患者进行的FLIPI风险评估,对RM治疗对诱导治疗的疗效进行了回顾性分析。我们在2013年至2019年期间确定了93例每3个月接受RM≥4次剂量的患者(RM组),以及60例未接受RM或接受利妥昔单抗少于4次剂量的患者(对照组)。中位随访39个月后,整个人群的中位总生存期(OS)和PFS均未达到。与对照组相比,RM组的PFS显著延长(中位PFS NA vs 83.1个月,P = 0.00027)。将人群分为3个FLIPI风险组时,各组PFS差异显著(4年PFS率,97.5% vs 88.8% vs 72.3%, P = 0.01)。与对照组相比,FLIPI低危RM患者的PFS无显著差异(4年PFS率,100% vs 93.8%, P = 0.23)。然而,RM组的FLIPI中危患者(4年PFS率,100% vs 70.3%, P = 0.00077)和高危患者(4年PFS率,86.7% vs 57.1%, P = 0.023)的PFS明显延长。这些数据表明,标准RM可显著延长中高风险FLIPI组患者的PFS,但不能延长低风险FLIPI组患者的PFS,有待更大规模的研究来验证。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


