{"title":"Olanzapine treatment effectively relieves breakthrough chemotherapy-induced nausea and vomiting: a real-world experience.","authors":"Akihiro Uchiike, Haruka Kono, Katsuhiro Miura, Tatsuya Hayama, Daisuke Tsutsumi, Shinya Tsuboi, Susumu Ohtsuka, Shinji Hidaka","doi":"10.1186/s40780-023-00293-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Olanzapine treatment prevents chemotherapy-induced nausea and vomiting (CINV) in patients receiving highly emetogenic chemotherapy (HEC). However, its role in the secondary prevention of breakthrough CINV in real-world cancer care should be further evaluated.</p><p><strong>Method: </strong>We conducted a retrospective study on patients receiving olanzapine to prevent breakthrough CINV refractory to standard antiemetic therapy. The major outcome was improvement in CINV, defined as any downgrade in CINV symptoms, according to the Common Terminology Criteria for Adverse Events. Comprete response was defined as no symptoms in CINV, i.e., Grade 0. These outcomes were compared in the HEC versus non-HEC groups and the standard- (5 or 10 mg/day) versus low- (2.5 mg/day) dose groups. The other outcome measurement was adverse events (AEs).</p><p><strong>Results: </strong>We analyzed 127 patients, including 92 women, with a median age of 50 years (range: 19-89 years). Baseline CINV severity was grade 1, 2, and 3 in 18%, 69%, and 13% of the patients, respectively. After prophylaxis with olanzapine at doses of 2.5, 5, or 10 mg/day, improvement was observed in 105 (83%) patients, with a complete response in 42 patients (33%). The improvement and complete remission rates for the HEC (n = 96) and non-HEC (n = 31) groups were 86% and 71% (p = 0.048) versus 38% and 19% (p = 0.062), respectively. The rates for the standard- (n = 98) and low- (n = 29) dose groups were 86% and 82% (p = 0.568) versus 28% and 52% (p = 0.015), respectively. Thirty-four patients (27%) experienced olanzapine-related AEs, mainly somnolence (n = 28). Grade 3 or higher AEs were not observed.</p><p><strong>Conclusion: </strong>Our study results support the clinical application of olanzapine for the secondary prevention of breakthrough CINV.</p>","PeriodicalId":16730,"journal":{"name":"Journal of Pharmaceutical Health Care and Sciences","volume":"9 1","pages":"24"},"PeriodicalIF":1.2000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10391758/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pharmaceutical Health Care and Sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40780-023-00293-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Olanzapine treatment prevents chemotherapy-induced nausea and vomiting (CINV) in patients receiving highly emetogenic chemotherapy (HEC). However, its role in the secondary prevention of breakthrough CINV in real-world cancer care should be further evaluated.
Method: We conducted a retrospective study on patients receiving olanzapine to prevent breakthrough CINV refractory to standard antiemetic therapy. The major outcome was improvement in CINV, defined as any downgrade in CINV symptoms, according to the Common Terminology Criteria for Adverse Events. Comprete response was defined as no symptoms in CINV, i.e., Grade 0. These outcomes were compared in the HEC versus non-HEC groups and the standard- (5 or 10 mg/day) versus low- (2.5 mg/day) dose groups. The other outcome measurement was adverse events (AEs).
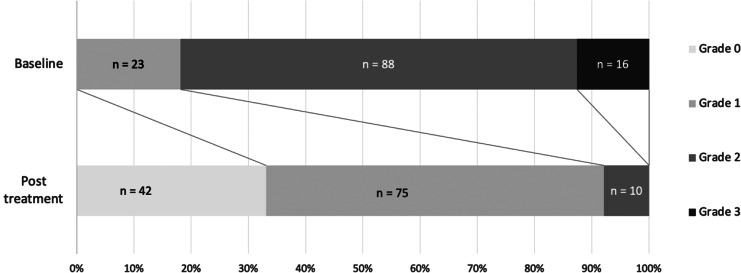
Results: We analyzed 127 patients, including 92 women, with a median age of 50 years (range: 19-89 years). Baseline CINV severity was grade 1, 2, and 3 in 18%, 69%, and 13% of the patients, respectively. After prophylaxis with olanzapine at doses of 2.5, 5, or 10 mg/day, improvement was observed in 105 (83%) patients, with a complete response in 42 patients (33%). The improvement and complete remission rates for the HEC (n = 96) and non-HEC (n = 31) groups were 86% and 71% (p = 0.048) versus 38% and 19% (p = 0.062), respectively. The rates for the standard- (n = 98) and low- (n = 29) dose groups were 86% and 82% (p = 0.568) versus 28% and 52% (p = 0.015), respectively. Thirty-four patients (27%) experienced olanzapine-related AEs, mainly somnolence (n = 28). Grade 3 or higher AEs were not observed.
Conclusion: Our study results support the clinical application of olanzapine for the secondary prevention of breakthrough CINV.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


