Davide Bizzoca, Andrea Piazzolla, Lorenzo Moretti, Giovanni Vicenti, Biagio Moretti, Giuseppe Solarino
{"title":"Physiologic postoperative presepsin kinetics following primary cementless total hip arthroplasty: A prospective observational study.","authors":"Davide Bizzoca, Andrea Piazzolla, Lorenzo Moretti, Giovanni Vicenti, Biagio Moretti, Giuseppe Solarino","doi":"10.5312/wjo.v14.i7.547","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Presepsin is an emerging biomarker in the diagnosis of sepsis. In the field of orthopaedics, it could be useful in diagnosing and managing periprosthetic joint infections.</p><p><strong>Aim: </strong>To define the normal postoperative presepsin plasmatic curve, in patients undergoing primary cementless total hip arthroplasty (THA).</p><p><strong>Methods: </strong>Patients undergoing primary cementless THA at our Institute were recruited. Inclusion criteria were: Primary osteoarthritis of the hip; urinary catheter time of permanence < 24 h; peripheral venous cannulation time of permanence < 24 h; no postoperative homologous blood transfusion administration and hospital stay ≤ 8 d. Exclusion criteria were: The presence of other articular prosthetic replacement or bone fixation devices; chronic inflammatory diseases; chronic kidney diseases; history of recurrent infections or malignant neoplasms; previous surgery in the preceding 12 mo; diabetes mellitus; immunosuppressive drug or corticosteroid assumption. All the patients received the same antibiotic prophylaxis. All the THA were performed by the same surgical and anaesthesia team; total operative time was defined as the time taken from skin incision to completion of skin closure. At enrollment, anthropometric data, smocking status, osteoarthritis stage according to Kellgren and Lawrence, Harris Hip Score, drugs assumption and comorbidities were recorded. All the patients underwent serial blood tests, including complete blood count, presepsin (PS) and C-reactive protein 24 h before arthroplasty and at 24, 48, 72 and 96 h postoperatively and at 3, 6 and 12-mo follow-up.</p><p><strong>Results: </strong>A total of 96 patients (51 female; 45 male; mean age = 65.74 ± 5.58) were recruited. The mean PS values were: 137.54 pg/mL at baseline, 192.08 pg/mL at 24 h post-op; 254.85 pg/mL at 48 h post-op; 259 pg/mL at 72 h post-op; 248.6 pg/mL at 96-h post-op; 140.52 pg/mL at 3-mo follow-up; 135.55 pg/mL at 6-mo follow-up and 130.11 pg/mL at 12-mo follow-up. In two patients (2.08%) a soft-tissue infection was observed; in these patients, higher levels (> 350 pg/mL) were recorded at 3-mo follow-up.</p><p><strong>Conclusion: </strong>The dosage of plasmatic PS concentration is highly recommended in patients undergoing THA before surgery to exclude the presence of an unknown infection. The PS plasmatic concentration should be also assessed at 72 h post-operatively, evaluate the maximum postoperative PS value, and at 96 h post-operatively when a decrease of presepsin should be found. The lack of a presepsin decrease at 96 h post-operatively could be a predictive factor of infection.</p>","PeriodicalId":47843,"journal":{"name":"World Journal of Orthopedics","volume":"14 7","pages":"547-553"},"PeriodicalIF":2.0000,"publicationDate":"2023-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/dd/16/WJO-14-547.PMC10359746.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Orthopedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5312/wjo.v14.i7.547","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Presepsin is an emerging biomarker in the diagnosis of sepsis. In the field of orthopaedics, it could be useful in diagnosing and managing periprosthetic joint infections.
Aim: To define the normal postoperative presepsin plasmatic curve, in patients undergoing primary cementless total hip arthroplasty (THA).
Methods: Patients undergoing primary cementless THA at our Institute were recruited. Inclusion criteria were: Primary osteoarthritis of the hip; urinary catheter time of permanence < 24 h; peripheral venous cannulation time of permanence < 24 h; no postoperative homologous blood transfusion administration and hospital stay ≤ 8 d. Exclusion criteria were: The presence of other articular prosthetic replacement or bone fixation devices; chronic inflammatory diseases; chronic kidney diseases; history of recurrent infections or malignant neoplasms; previous surgery in the preceding 12 mo; diabetes mellitus; immunosuppressive drug or corticosteroid assumption. All the patients received the same antibiotic prophylaxis. All the THA were performed by the same surgical and anaesthesia team; total operative time was defined as the time taken from skin incision to completion of skin closure. At enrollment, anthropometric data, smocking status, osteoarthritis stage according to Kellgren and Lawrence, Harris Hip Score, drugs assumption and comorbidities were recorded. All the patients underwent serial blood tests, including complete blood count, presepsin (PS) and C-reactive protein 24 h before arthroplasty and at 24, 48, 72 and 96 h postoperatively and at 3, 6 and 12-mo follow-up.
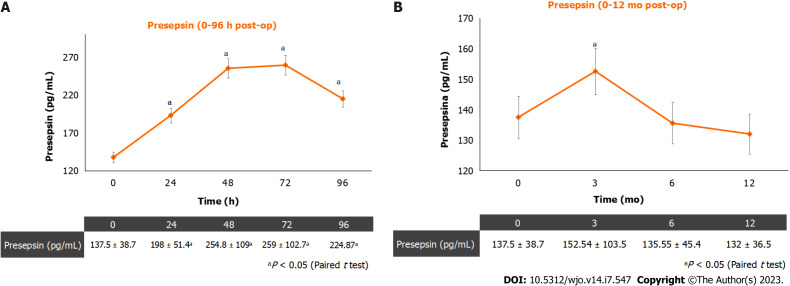
Results: A total of 96 patients (51 female; 45 male; mean age = 65.74 ± 5.58) were recruited. The mean PS values were: 137.54 pg/mL at baseline, 192.08 pg/mL at 24 h post-op; 254.85 pg/mL at 48 h post-op; 259 pg/mL at 72 h post-op; 248.6 pg/mL at 96-h post-op; 140.52 pg/mL at 3-mo follow-up; 135.55 pg/mL at 6-mo follow-up and 130.11 pg/mL at 12-mo follow-up. In two patients (2.08%) a soft-tissue infection was observed; in these patients, higher levels (> 350 pg/mL) were recorded at 3-mo follow-up.
Conclusion: The dosage of plasmatic PS concentration is highly recommended in patients undergoing THA before surgery to exclude the presence of an unknown infection. The PS plasmatic concentration should be also assessed at 72 h post-operatively, evaluate the maximum postoperative PS value, and at 96 h post-operatively when a decrease of presepsin should be found. The lack of a presepsin decrease at 96 h post-operatively could be a predictive factor of infection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


