Amarpreet Bhalla , Qiang Liu , Yanan Fang , Jay H Lefkowitch
{"title":"IgG4 plasma cell neoplasm in liver transplant biopsy masquerading as rejection","authors":"Amarpreet Bhalla , Qiang Liu , Yanan Fang , Jay H Lefkowitch","doi":"10.1016/j.lrr.2023.100379","DOIUrl":null,"url":null,"abstract":"<div><p>IgG4 plasma cell neoplasm and myeloma are rare disease entities, not associated with systemic fibroinflammatory IgG4 related disease. We herein present a case of IgG4 plasma cell neoplasm in a liver transplant biopsy. A 55 year old female was treated with living donor transplant and had a complicated post-operative course. Three months post-transplant, she presented with small for size syndrome, biliary stricture, and inferior vena cava stenosis. Concomitant liver biopsy revealed mild acute cellular rejection with central perivenulitis pattern, and mild centrilobular fibrosis. She was treated with steroids which resulted in improvement of liver enzymes. Seven months post-transplant, she presented with subtherapeutic prograf levels and cholestatic pattern of elevated liver tests. ERCP revealed a stone which was removed. Hematological evaluation revealed an abnormal serum protein electrophoresis (SPEP). Monoclonal IgG kappa was elevated along with mildly elevated free Kappa/Lambda ratio. She was followed up and readmitted two months later for worsening liver function tests. The liver biopsy showed monotypic Kappa-and IgG4-restricted plasma cell infiltrates in portal, periportal, sinusoidal and centrilobular regions, compatible with plasma cell neoplasm. In the clinical context of positivity for a serum M-spike, the monoclonal hepatic infiltrates were deemed consistent with a Kappa-and IgG4-restricted plasma cell neoplasm. Patient was treated with pulsed steroids, and liver function tests subsequently downtrended. She was followed up by Hemoncology, and the treatment plan included carfilzomib-based induction therapy and dexamethasone to prevent end-organ damage from evolving myeloma. In the meanwhile, she developed acute appendicitis, underwent appendectomy, and passed away in the post-operative period.</p></div>","PeriodicalId":38435,"journal":{"name":"Leukemia Research Reports","volume":null,"pages":null},"PeriodicalIF":0.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/87/99/main.PMC10371806.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Leukemia Research Reports","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2213048923000195","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
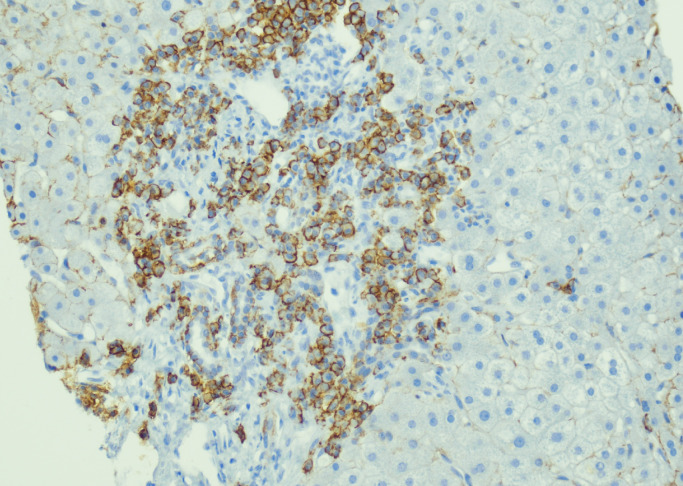
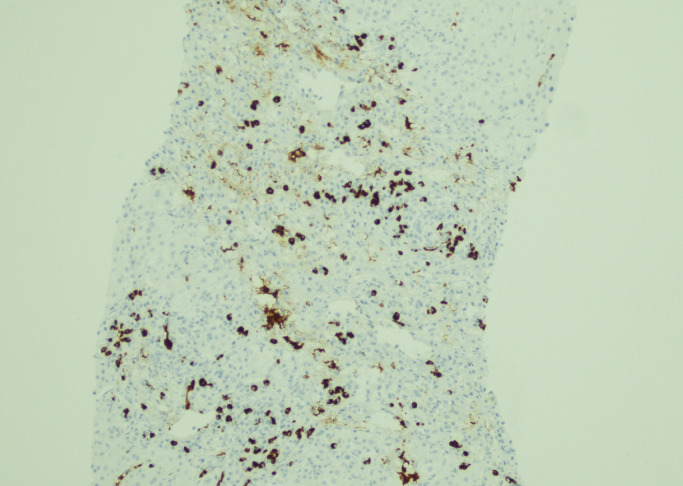
IgG4 plasma cell neoplasm and myeloma are rare disease entities, not associated with systemic fibroinflammatory IgG4 related disease. We herein present a case of IgG4 plasma cell neoplasm in a liver transplant biopsy. A 55 year old female was treated with living donor transplant and had a complicated post-operative course. Three months post-transplant, she presented with small for size syndrome, biliary stricture, and inferior vena cava stenosis. Concomitant liver biopsy revealed mild acute cellular rejection with central perivenulitis pattern, and mild centrilobular fibrosis. She was treated with steroids which resulted in improvement of liver enzymes. Seven months post-transplant, she presented with subtherapeutic prograf levels and cholestatic pattern of elevated liver tests. ERCP revealed a stone which was removed. Hematological evaluation revealed an abnormal serum protein electrophoresis (SPEP). Monoclonal IgG kappa was elevated along with mildly elevated free Kappa/Lambda ratio. She was followed up and readmitted two months later for worsening liver function tests. The liver biopsy showed monotypic Kappa-and IgG4-restricted plasma cell infiltrates in portal, periportal, sinusoidal and centrilobular regions, compatible with plasma cell neoplasm. In the clinical context of positivity for a serum M-spike, the monoclonal hepatic infiltrates were deemed consistent with a Kappa-and IgG4-restricted plasma cell neoplasm. Patient was treated with pulsed steroids, and liver function tests subsequently downtrended. She was followed up by Hemoncology, and the treatment plan included carfilzomib-based induction therapy and dexamethasone to prevent end-organ damage from evolving myeloma. In the meanwhile, she developed acute appendicitis, underwent appendectomy, and passed away in the post-operative period.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


