{"title":"Review of the Pathophysiologic and Clinical Aspects of Hypokalemia in Children and Young Adults: an Update.","authors":"Oluwatoyin Fatai Bamgbola","doi":"10.1007/s40746-022-00240-3","DOIUrl":null,"url":null,"abstract":"<p><p>This article examines the regulatory function of the skeletal muscle, renal, and adrenergic systems in potassium homeostasis. The pathophysiologic bases of hypokalemia, systematic approach for an early diagnosis, and therapeutic strategy to avert life-threatening complications are highlighted. By promoting skeletal muscle uptake, intense physical exercise (post), severe trauma, and several toxins produce profound hypokalemia. Hypovolemia due to renal and extra-renal fluid losses and ineffective circulation activate secondary aldosteronism causing urinary potassium wasting. In addition to hypokalemic alkalosis, primary aldosteronism causes low-renin hypertension. Non-aldosterone mineralocorticoid activation leading to low-renin and low-aldosterone hypertension occurs in Liddle's syndrome and apparent mineralocorticoid excess. Although there is enzymatic inhibition of cortisol synthesis in congenital adrenal hyperplasia, precursors of aldosterone produce low-renin hypokalemic hypertension. In addition to the glucocorticoid effect, hypercortisolism activates mineralocorticoid receptors in Cushing's syndrome. Genetic mutations involving furosemide-sensitive Na<sup>+</sup>-K<sup>+</sup>-2Cl<sup>-</sup> co-transporters and thiazide-sensitive Na<sup>+</sup>-Cl<sup>-</sup> transporters result in (non-hypertensive) salt-wasting nephropathy. Proximal and distal renal tubular acidosis is associated with hypokalemia. Eating disorders causing hypokalemia include bulimia, laxative abuse, and diuretic misuse. Low urinary potassium (<15 mmol/day) and/or low urinary chloride (<20 mol/L) suggest a gastrointestinal pathology. Co-morbidity of hypokalemia with chronic pulmonary and cardiovascular diseases may increase the fatality rate.</p>","PeriodicalId":37445,"journal":{"name":"Current Treatment Options in Pediatrics","volume":"8 3","pages":"96-114"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9115742/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Treatment Options in Pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40746-022-00240-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/5/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
Abstract
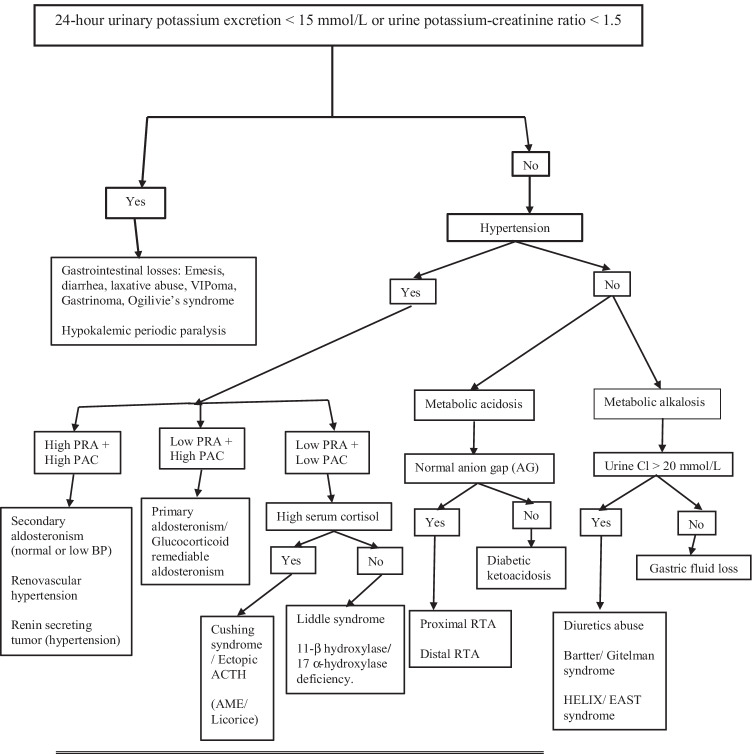
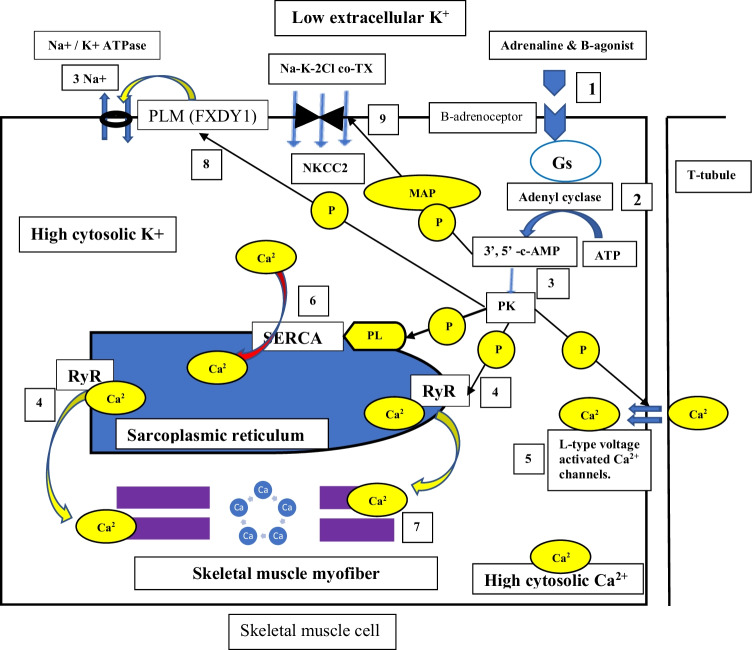
This article examines the regulatory function of the skeletal muscle, renal, and adrenergic systems in potassium homeostasis. The pathophysiologic bases of hypokalemia, systematic approach for an early diagnosis, and therapeutic strategy to avert life-threatening complications are highlighted. By promoting skeletal muscle uptake, intense physical exercise (post), severe trauma, and several toxins produce profound hypokalemia. Hypovolemia due to renal and extra-renal fluid losses and ineffective circulation activate secondary aldosteronism causing urinary potassium wasting. In addition to hypokalemic alkalosis, primary aldosteronism causes low-renin hypertension. Non-aldosterone mineralocorticoid activation leading to low-renin and low-aldosterone hypertension occurs in Liddle's syndrome and apparent mineralocorticoid excess. Although there is enzymatic inhibition of cortisol synthesis in congenital adrenal hyperplasia, precursors of aldosterone produce low-renin hypokalemic hypertension. In addition to the glucocorticoid effect, hypercortisolism activates mineralocorticoid receptors in Cushing's syndrome. Genetic mutations involving furosemide-sensitive Na+-K+-2Cl- co-transporters and thiazide-sensitive Na+-Cl- transporters result in (non-hypertensive) salt-wasting nephropathy. Proximal and distal renal tubular acidosis is associated with hypokalemia. Eating disorders causing hypokalemia include bulimia, laxative abuse, and diuretic misuse. Low urinary potassium (<15 mmol/day) and/or low urinary chloride (<20 mol/L) suggest a gastrointestinal pathology. Co-morbidity of hypokalemia with chronic pulmonary and cardiovascular diseases may increase the fatality rate.
期刊介绍:
Current Treatment Options in Pediatrics aims to review the most important, recently published research on treatment in the field of pediatrics. By providing clear, insightful, balanced contributions by international experts, the journal intends to serve all those involved in the care of children of all ages.We accomplish this aim by appointing international authorities to serve as Section Editors in key subject areas covering all the major medical and surgical disciplines in pediatrics. Section Editors, in turn, select topics for which leading experts contribute comprehensive treatment-focused review articles that emphasize new developments and recently published papers of major importance, highlighted by annotated reference lists. An international Editorial Board reviews the annual table of contents, suggests articles of special interest to their country/region, and ensures that topics are current and include emerging research. Commentaries from well-known figures in the field are also occasionally provided.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


