An Updated Meta-Analysis on Cerebral Embolic Protection in Patients Undergoing Transcatheter Aortic Valve Intervention Stratified by Baseline Surgical Risk and Device Type
Safi U. Khan MD, MS , Salman Zahid MD , Mohamad A. Alkhouli MD , Usman Ali Akbar MD , Syed Zaid MD , Hassaan B. Arshad MD , Stephen H. Little MD , Michael J. Reardon MD , Neal S. Kleiman MD , Sachin S. Goel MD
{"title":"An Updated Meta-Analysis on Cerebral Embolic Protection in Patients Undergoing Transcatheter Aortic Valve Intervention Stratified by Baseline Surgical Risk and Device Type","authors":"Safi U. Khan MD, MS , Salman Zahid MD , Mohamad A. Alkhouli MD , Usman Ali Akbar MD , Syed Zaid MD , Hassaan B. Arshad MD , Stephen H. Little MD , Michael J. Reardon MD , Neal S. Kleiman MD , Sachin S. Goel MD","doi":"10.1016/j.shj.2023.100178","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Transcatheter aortic valve intervention (TAVI) can lead to the embolization of debris. Capturing the debris by cerebral embolic protection (CEP) devices may reduce the risk of stroke. New evidence has allowed us to examine the effects of CEP in patients undergoing TAVI. We aimed to assess the effects of CEP overall and stratified by the device used (SENTINEL or TriGuard) and the surgical risk of the patients.</p></div><div><h3>Methods</h3><p>We selected randomized controlled trials using electronic databases through September 17, 2022. We estimated random-effects risk ratios (RR) with (95% confidence interval) and calculated absolute risk differences at 30 days across baseline surgical risks derived from the TAVI trials for any stroke (disabling and nondisabling) and all-cause mortality.</p></div><div><h3>Results</h3><p>Among 6 trials (n = 3921), CEP vs. control did not reduce any stroke [RR: 0.95 (0.50-1.81)], disabling [RR: 0.75 (0.18-3.16)] or nondisabling [RR: 0.99 (0.65-1.49)] strokes, or all-cause mortality [RR: 1.23 (0.55-2.77)]. However, when analyzed by device, SENTINEL reduced disabling stroke [RR: 0.46 (0.22-0.95)], translating into 6 fewer per 1000 in high-risk, 3 fewer per 1000 in intermediate-risk, and 1 fewer per 1000 in low surgical-risk patients. CEP vs. control did not reduce the risk of any bleeding [RR: 1.03 (0.44-2.40)], major vascular complications [RR: 1.41 (0.57-3.48)], or acute kidney injury [RR: 1.36 (0.57-3.28)].</p></div><div><h3>Conclusions</h3><p>This updated meta-analysis showed that SENTINEL CEP might reduce disabling stroke in patients undergoing TAVI. Patients with high and intermediate surgical risks were most likely to derive benefits.</p></div>","PeriodicalId":36053,"journal":{"name":"Structural Heart","volume":"7 4","pages":"Article 100178"},"PeriodicalIF":1.4000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10382981/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Structural Heart","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2474870623000404","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Transcatheter aortic valve intervention (TAVI) can lead to the embolization of debris. Capturing the debris by cerebral embolic protection (CEP) devices may reduce the risk of stroke. New evidence has allowed us to examine the effects of CEP in patients undergoing TAVI. We aimed to assess the effects of CEP overall and stratified by the device used (SENTINEL or TriGuard) and the surgical risk of the patients.
Methods
We selected randomized controlled trials using electronic databases through September 17, 2022. We estimated random-effects risk ratios (RR) with (95% confidence interval) and calculated absolute risk differences at 30 days across baseline surgical risks derived from the TAVI trials for any stroke (disabling and nondisabling) and all-cause mortality.
Results
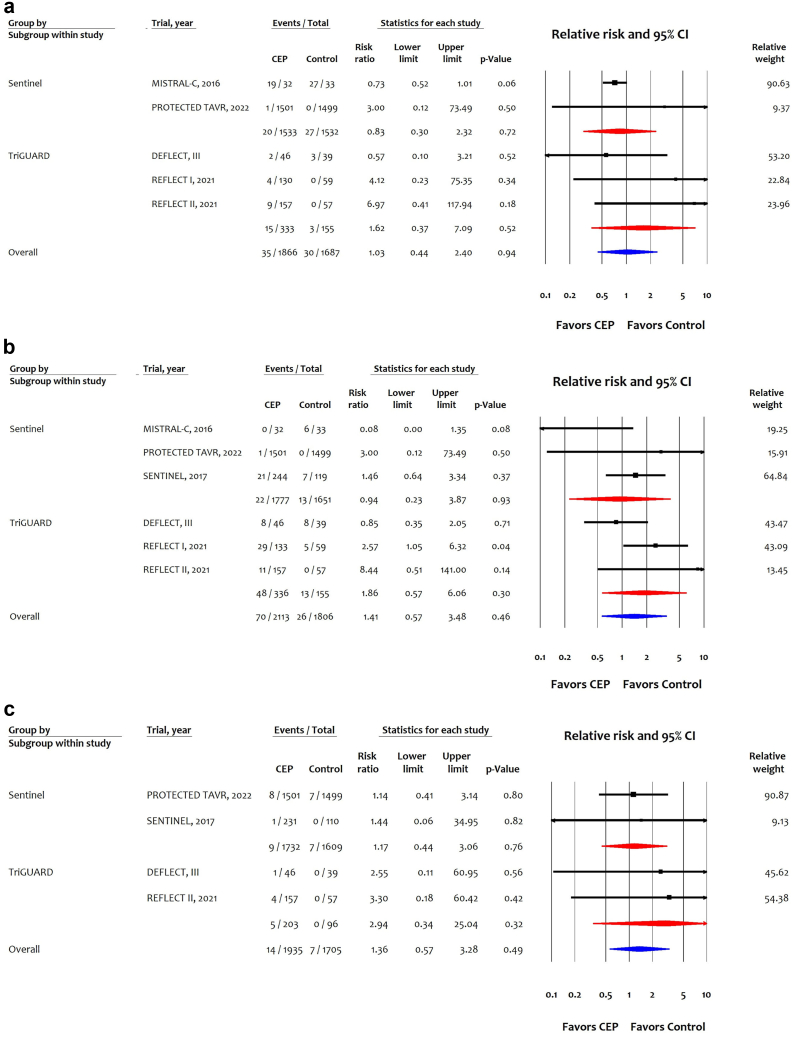
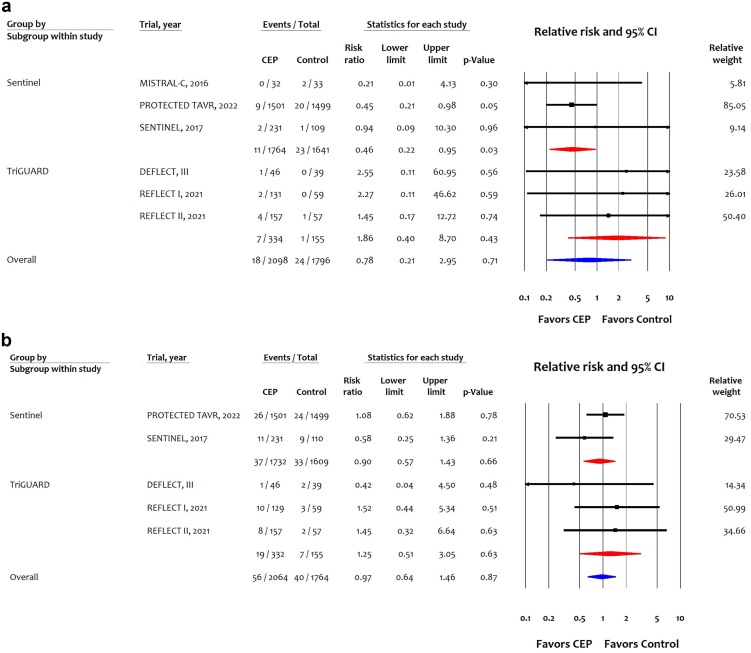
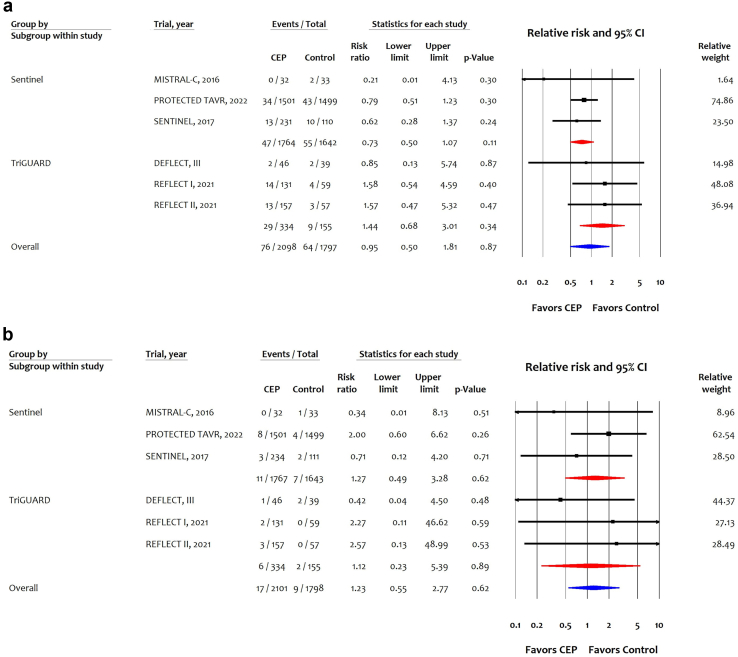
Among 6 trials (n = 3921), CEP vs. control did not reduce any stroke [RR: 0.95 (0.50-1.81)], disabling [RR: 0.75 (0.18-3.16)] or nondisabling [RR: 0.99 (0.65-1.49)] strokes, or all-cause mortality [RR: 1.23 (0.55-2.77)]. However, when analyzed by device, SENTINEL reduced disabling stroke [RR: 0.46 (0.22-0.95)], translating into 6 fewer per 1000 in high-risk, 3 fewer per 1000 in intermediate-risk, and 1 fewer per 1000 in low surgical-risk patients. CEP vs. control did not reduce the risk of any bleeding [RR: 1.03 (0.44-2.40)], major vascular complications [RR: 1.41 (0.57-3.48)], or acute kidney injury [RR: 1.36 (0.57-3.28)].
Conclusions
This updated meta-analysis showed that SENTINEL CEP might reduce disabling stroke in patients undergoing TAVI. Patients with high and intermediate surgical risks were most likely to derive benefits.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


