Yang Lei, Jennifer Halasz, Kerri L Novak, Stephen E Congly
{"title":"Intermittent Proton Pump Inhibitor Therapy in Low-Risk Non-Variceal Upper Gastrointestinal Bleeding May Be Significantly Cost-Saving.","authors":"Yang Lei, Jennifer Halasz, Kerri L Novak, Stephen E Congly","doi":"10.3390/medicines10070044","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>High-dose proton pump inhibitor (PPI) therapy, given either intermittently or continuously for non-variceal upper gastrointestinal bleeding (NV-UGIB), is efficacious. Using intermittent PPI for low-risk patients may be cost-saving. Our objective was to estimate the annual cost savings if all low-risk NV-UGIB patients received intermittent PPI therapy.</p><p><strong>Methods: </strong>Patients who presented to hospital in Calgary, Alberta, who received a PPI for NV-UGIB from July 2015 to March 2017 were identified using ICD-10 codes. Patients were stratified into no endoscopy, high-risk, and low-risk lesion groups and further subdivided into no PPI, oral PPI, intermittent intravenous (IV), and continuous IV subgroups. Average length of stay (LOS) in each subgroup and costs were calculated.</p><p><strong>Results: </strong>We identified 4141 patients with NV-UGIBs, (median age 61, 57.4% male). One-thousand two-hundred and thirty-one low-risk patients received continuous IV PPI, with an average LOS of 6.8 days (95% CI 6.2-7.3) versus 4.9 days (95% CI 3.9-5.9) for intermittent IV patients. If continuous IV PPI patients instead received intermittent IV PPI, 3852 patient days and CAD 11,714,390 (2017 CAD)/year could be saved.</p><p><strong>Conclusions: </strong>Using real-world administrative data, we demonstrate that a sizable portion of low-risk patients with NV-UGIB who were given continuous IV PPI if switched to intermittent IV therapy could generate significant potential cost savings.</p>","PeriodicalId":74162,"journal":{"name":"Medicines (Basel, Switzerland)","volume":"10 7","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-07-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10384205/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medicines (Basel, Switzerland)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/medicines10070044","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: High-dose proton pump inhibitor (PPI) therapy, given either intermittently or continuously for non-variceal upper gastrointestinal bleeding (NV-UGIB), is efficacious. Using intermittent PPI for low-risk patients may be cost-saving. Our objective was to estimate the annual cost savings if all low-risk NV-UGIB patients received intermittent PPI therapy.
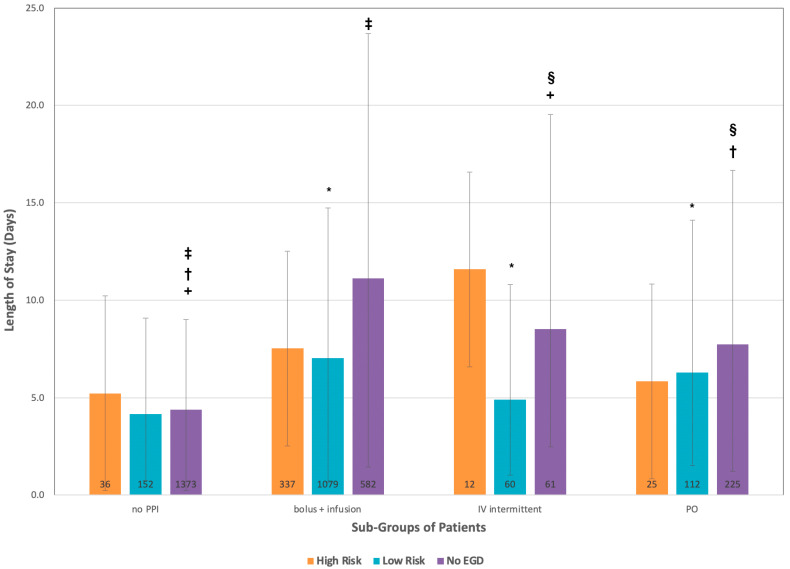
Methods: Patients who presented to hospital in Calgary, Alberta, who received a PPI for NV-UGIB from July 2015 to March 2017 were identified using ICD-10 codes. Patients were stratified into no endoscopy, high-risk, and low-risk lesion groups and further subdivided into no PPI, oral PPI, intermittent intravenous (IV), and continuous IV subgroups. Average length of stay (LOS) in each subgroup and costs were calculated.
Results: We identified 4141 patients with NV-UGIBs, (median age 61, 57.4% male). One-thousand two-hundred and thirty-one low-risk patients received continuous IV PPI, with an average LOS of 6.8 days (95% CI 6.2-7.3) versus 4.9 days (95% CI 3.9-5.9) for intermittent IV patients. If continuous IV PPI patients instead received intermittent IV PPI, 3852 patient days and CAD 11,714,390 (2017 CAD)/year could be saved.
Conclusions: Using real-world administrative data, we demonstrate that a sizable portion of low-risk patients with NV-UGIB who were given continuous IV PPI if switched to intermittent IV therapy could generate significant potential cost savings.
背景:间歇或连续给予大剂量质子泵抑制剂(PPI)治疗非静脉曲张性上消化道出血(NV-UGIB)是有效的。对低风险患者使用间歇性PPI可能节省成本。我们的目的是估计如果所有低风险NV-UGIB患者接受间歇性PPI治疗,每年节省的费用。方法:使用ICD-10代码对2015年7月至2017年3月在阿尔伯塔省卡尔加里医院接受过NV-UGIB PPI治疗的患者进行识别。将患者分为无内镜检查组、高危组和低危组,并进一步细分为无PPI组、口服PPI组、间歇静脉注射组和持续静脉注射组。计算每个亚组的平均住院时间(LOS)和费用。结果:我们确定了4141例NV-UGIBs患者,(中位年龄61岁,男性57.4%)。1231名低危患者接受持续静脉注射PPI,平均生存期为6.8天(95% CI 6.2-7.3),而间歇静脉注射患者为4.9天(95% CI 3.9-5.9)。如果将持续静脉注射PPI的患者改为间歇性静脉注射PPI,可节省3852个患者日和11,714,390加元(2017加元)/年。结论:使用现实世界的管理数据,我们证明了相当一部分低风险的NV-UGIB患者,如果将持续静脉注射PPI改为间歇性静脉注射治疗,可以产生显着的潜在成本节约。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


