{"title":"Progression from prediabetes to type 2 diabetes mellitus in adolescents: a real world experience.","authors":"Alyson Weiner, Meng Zhang, Sheng Ren, Beverly Tchang, Rachelle Gandica, Jaime Murillo","doi":"10.3389/fcdhc.2023.1181729","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Obesity in pediatric patients is strongly associated with increased vascular and metabolic risk. Prediabetes is present in up to 1 in 5 adolescents, aged 12-18 years-old, though is thought to remit spontaneously in a significant portion. Pediatric patients with type 2 diabetes mellitus (T2D) have a more rapid decline of beta-cell function and progression to treatment failure than adult T2D patients. Thus, there is a strong interest in better understanding the natural history of prediabetes in these youth. We aimed to evaluate the real-world rate of progression of prediabetes to T2D in adolescent patients.</p><p><strong>Methods: </strong>This is a retrospective study of 9,275 adolescent subjects aged 12-21 years-old with at least 3 years of de-identified commercial claims data and a new diagnosis of prediabetes during the observation period. Enrollees with a T2D diagnosis and/or diabetes medication use in the 1 year prior to prediabetes diagnosis or a T2D diagnosis in the 1 month following prediabetes diagnosis were excluded. Enrollees with diagnoses of type 1 diabetes (T1D) or polycystic ovarian syndrome over the 3 years were also excluded. Progression to T2D was defined by claims data of two T2D diagnoses at least 7 days apart, HbA1c ≥ 6.5%, and/or prescription of insulin without known T1D. Enrollees were followed for 2 years after prediabetes diagnosis.</p><p><strong>Results: </strong>Overall, 232 subjects (2.5%) progressed from prediabetes to T2D. There were no differences found in T2D progression based on sex or age. Progression to T2D occurred at a median of 302 days after prediabetes diagnosis (IQR 123 to 518 days). This study was limited by the lack of laboratory/anthropometric data in administrative claims, as well as the exclusion of 23,825 enrollees for lack of continuous commercial claims data over 3 years.</p><p><strong>Conclusion: </strong>In the largest sample to date on adolescent prediabetes, we found a 2.5% progression of prediabetes to T2D over a median duration of about one year.</p>","PeriodicalId":73075,"journal":{"name":"Frontiers in clinical diabetes and healthcare","volume":"4 ","pages":"1181729"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10204924/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in clinical diabetes and healthcare","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fcdhc.2023.1181729","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Obesity in pediatric patients is strongly associated with increased vascular and metabolic risk. Prediabetes is present in up to 1 in 5 adolescents, aged 12-18 years-old, though is thought to remit spontaneously in a significant portion. Pediatric patients with type 2 diabetes mellitus (T2D) have a more rapid decline of beta-cell function and progression to treatment failure than adult T2D patients. Thus, there is a strong interest in better understanding the natural history of prediabetes in these youth. We aimed to evaluate the real-world rate of progression of prediabetes to T2D in adolescent patients.
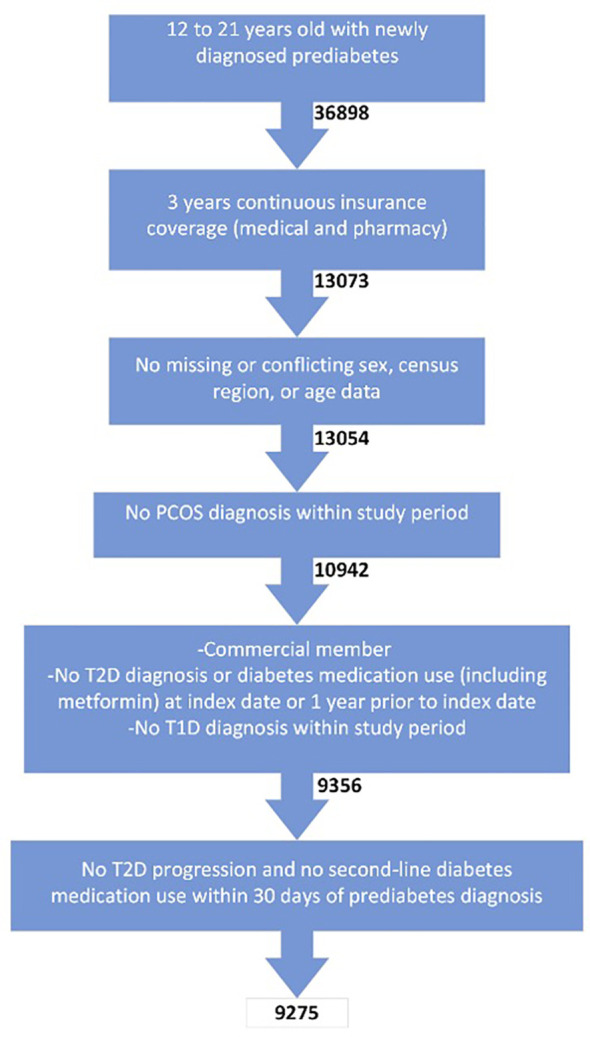
Methods: This is a retrospective study of 9,275 adolescent subjects aged 12-21 years-old with at least 3 years of de-identified commercial claims data and a new diagnosis of prediabetes during the observation period. Enrollees with a T2D diagnosis and/or diabetes medication use in the 1 year prior to prediabetes diagnosis or a T2D diagnosis in the 1 month following prediabetes diagnosis were excluded. Enrollees with diagnoses of type 1 diabetes (T1D) or polycystic ovarian syndrome over the 3 years were also excluded. Progression to T2D was defined by claims data of two T2D diagnoses at least 7 days apart, HbA1c ≥ 6.5%, and/or prescription of insulin without known T1D. Enrollees were followed for 2 years after prediabetes diagnosis.
Results: Overall, 232 subjects (2.5%) progressed from prediabetes to T2D. There were no differences found in T2D progression based on sex or age. Progression to T2D occurred at a median of 302 days after prediabetes diagnosis (IQR 123 to 518 days). This study was limited by the lack of laboratory/anthropometric data in administrative claims, as well as the exclusion of 23,825 enrollees for lack of continuous commercial claims data over 3 years.
Conclusion: In the largest sample to date on adolescent prediabetes, we found a 2.5% progression of prediabetes to T2D over a median duration of about one year.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


