{"title":"Time-series comparison of COVID-19 case fatality rates across 21 countries with adjustment for multiple covariates.","authors":"Yongmoon Kim, Bryan Inho Kim, Sangwoo Tak","doi":"10.24171/j.phrp.2022.0212","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Although it is widely used as a measure for mortality, the case fatality rate (CFR) ofcoronavirus disease 2019 (COVID-19) can vary over time and fluctuate for many reasons otherthan viral characteristics. To compare the CFRs of different countries in equal measure, weestimated comparable CFRs after adjusting for multiple covariates and examined the mainfactors that contributed to variability in the CFRs among 21 countries.</p><p><strong>Methods: </strong>For statistical analysis, time-series cross-sectional data were collected from OurWorld in Data, CoVariants.org, and GISAID. Biweekly CFRs of COVID-19 were estimated bypooled generalized linear squares regression models for the panel data. Covariates includedthe predominant virus variant, reproduction rate, vaccination, national economic status,hospital beds, diabetes prevalence, and population share of individuals older than age 65. Intotal, 21 countries were eligible for analysis.</p><p><strong>Results: </strong>Adjustment for covariates reduced variation in the CFRs of COVID-19 across countriesand over time. Regression results showed that the dominant spread of the Omicron variant,reproduction rate, and vaccination were associated with lower country-level CFRs, whereasage, the extreme poverty rate, and diabetes prevalence were associated with higher countrylevel CFRs.</p><p><strong>Conclusion: </strong>A direct comparison of crude CFRs among countries may be fallacious, especiallyin a cross-sectional analysis. Our study presents an adjusted comparison of CFRs over timefor a more proper comparison. In addition, our findings suggest that comparing CFRs amongdifferent countries without considering their context, such as the epidemic phase, medicalcapacity, surveillance strategy, and socio-demographic traits, should be avoided.</p>","PeriodicalId":38949,"journal":{"name":"Osong Public Health and Research Perspectives","volume":"13 6","pages":"424-434"},"PeriodicalIF":2.1000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/03/b3/j-phrp-2022-0212.PMC10211436.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Osong Public Health and Research Perspectives","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.24171/j.phrp.2022.0212","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 1
Abstract
Objectives: Although it is widely used as a measure for mortality, the case fatality rate (CFR) ofcoronavirus disease 2019 (COVID-19) can vary over time and fluctuate for many reasons otherthan viral characteristics. To compare the CFRs of different countries in equal measure, weestimated comparable CFRs after adjusting for multiple covariates and examined the mainfactors that contributed to variability in the CFRs among 21 countries.
Methods: For statistical analysis, time-series cross-sectional data were collected from OurWorld in Data, CoVariants.org, and GISAID. Biweekly CFRs of COVID-19 were estimated bypooled generalized linear squares regression models for the panel data. Covariates includedthe predominant virus variant, reproduction rate, vaccination, national economic status,hospital beds, diabetes prevalence, and population share of individuals older than age 65. Intotal, 21 countries were eligible for analysis.
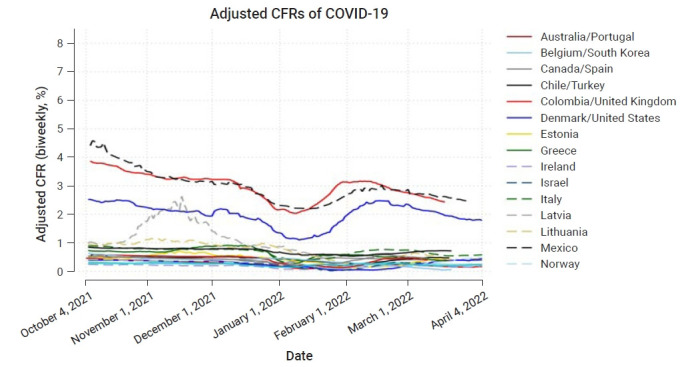
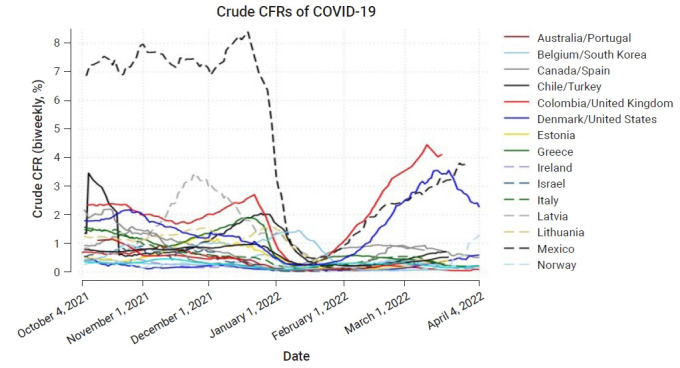
Results: Adjustment for covariates reduced variation in the CFRs of COVID-19 across countriesand over time. Regression results showed that the dominant spread of the Omicron variant,reproduction rate, and vaccination were associated with lower country-level CFRs, whereasage, the extreme poverty rate, and diabetes prevalence were associated with higher countrylevel CFRs.
Conclusion: A direct comparison of crude CFRs among countries may be fallacious, especiallyin a cross-sectional analysis. Our study presents an adjusted comparison of CFRs over timefor a more proper comparison. In addition, our findings suggest that comparing CFRs amongdifferent countries without considering their context, such as the epidemic phase, medicalcapacity, surveillance strategy, and socio-demographic traits, should be avoided.
虽然它被广泛用作死亡率的衡量标准,但2019年冠状病毒病(COVID-19)的病死率(CFR)可能会随着时间的推移而变化,并且由于病毒特征以外的许多原因而波动。为了在同等程度上比较不同国家的CFRs,我们在调整多个协变量后估计了可比较的CFRs,并检查了21个国家中导致CFRs变异的主要因素。方法:采用OurWorld in data、CoVariants.org和GISAID的时间序列截面数据进行统计分析。通过面板数据的合并广义线性平方回归模型估计COVID-19的双周cfr。协变量包括主要病毒变异、繁殖率、疫苗接种、国民经济状况、医院床位、糖尿病患病率和65岁以上人口比例。总共有21个国家有资格进行分析。结果:协变量的调整减少了COVID-19在不同国家和不同时期的cfr差异。回归结果显示,Omicron变异的显性传播、繁殖率和疫苗接种与较低的国家级CFRs相关,而年龄、极端贫困率和糖尿病患病率与较高的国家级CFRs相关。结论:直接比较各国之间的粗cfr可能是错误的,特别是在横断面分析中。我们的研究提出了一种调整后的CFRs随时间的比较,以便进行更适当的比较。此外,我们的研究结果表明,应避免在不考虑其背景(如流行阶段、医疗能力、监测策略和社会人口特征)的情况下比较不同国家的CFRs。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


