{"title":"Side-by-side deployment of gore excluder legs at a narrow terminal aorta for endovascular aneurysm repair.","authors":"Yu Hohri, Hidetake Kawajiri, Keiichi Kanda, Satoshi Numata, Takuma Kobayashi, Rie Nakai, Hitoshi Yaku","doi":"10.1007/s10047-023-01406-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>A narrow terminal aorta is a risk factor for endograft occlusion after endovascular aneurysm repair. To minimize limb complications, we used Gore Excluder legs positioned side-by-side at the terminal aorta. We investigated the outcomes of our strategy for endovascular aneurysm repair in patients with a narrow terminal aorta.</p><p><strong>Methods: </strong>We enrolled 61 patients who underwent endovascular aneurysm repair with a narrow terminal aorta (defined as < 18 mm in diameter) from April 2013 to October 2021. The standard procedure involves complete treatment with the Gore Excluder device. When other types of main body endografts were used, they were deployed proximal to the terminal aorta, and we used the Gore Excluder leg device in the bilateral limbs. Postoperatively, the intraluminal diameter of the legs at the terminal aorta was measured to assess the configuration.</p><p><strong>Results: </strong>During the follow-up period (mean: 2.7 ± 2.0 years), there were no aorta-related deaths, endograft occlusions, or leg-related re-interventions. There were no significant differences between the pre- and postoperative ankle-brachial pressure index values in the dominant and non-dominant legs (p = 0.44 and p = 0.17, respectively). Postoperatively, the mean difference rate (defined as [dominant leg diameter-non-dominant leg diameter]/terminal aorta diameter) was 7.5 ± 7.1%. The difference rate was not significantly correlated with the terminal aortic diameter, calcification thickness, or circumferential calcification (r = 0.16, p = 0.22; r = 0.07, p = 0.59; and r = - 0.07, p = 0.61, respectively).</p><p><strong>Conclusions: </strong>Side-by-side deployment of Gore Excluder legs produces acceptable outcomes for endovascular aneurysm repair with a narrow terminal aorta. The endograft expansion at the terminal aorta is tolerable without influencing calcification distribution.</p>","PeriodicalId":15177,"journal":{"name":"Journal of Artificial Organs","volume":" ","pages":"238-246"},"PeriodicalIF":1.3000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Artificial Organs","FirstCategoryId":"5","ListUrlMain":"https://doi.org/10.1007/s10047-023-01406-y","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/5/25 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ENGINEERING, BIOMEDICAL","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: A narrow terminal aorta is a risk factor for endograft occlusion after endovascular aneurysm repair. To minimize limb complications, we used Gore Excluder legs positioned side-by-side at the terminal aorta. We investigated the outcomes of our strategy for endovascular aneurysm repair in patients with a narrow terminal aorta.
Methods: We enrolled 61 patients who underwent endovascular aneurysm repair with a narrow terminal aorta (defined as < 18 mm in diameter) from April 2013 to October 2021. The standard procedure involves complete treatment with the Gore Excluder device. When other types of main body endografts were used, they were deployed proximal to the terminal aorta, and we used the Gore Excluder leg device in the bilateral limbs. Postoperatively, the intraluminal diameter of the legs at the terminal aorta was measured to assess the configuration.
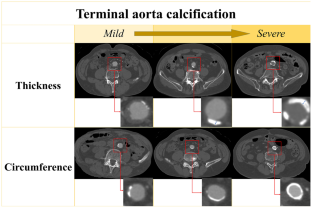
Results: During the follow-up period (mean: 2.7 ± 2.0 years), there were no aorta-related deaths, endograft occlusions, or leg-related re-interventions. There were no significant differences between the pre- and postoperative ankle-brachial pressure index values in the dominant and non-dominant legs (p = 0.44 and p = 0.17, respectively). Postoperatively, the mean difference rate (defined as [dominant leg diameter-non-dominant leg diameter]/terminal aorta diameter) was 7.5 ± 7.1%. The difference rate was not significantly correlated with the terminal aortic diameter, calcification thickness, or circumferential calcification (r = 0.16, p = 0.22; r = 0.07, p = 0.59; and r = - 0.07, p = 0.61, respectively).
Conclusions: Side-by-side deployment of Gore Excluder legs produces acceptable outcomes for endovascular aneurysm repair with a narrow terminal aorta. The endograft expansion at the terminal aorta is tolerable without influencing calcification distribution.
期刊介绍:
The aim of the Journal of Artificial Organs is to introduce to colleagues worldwide a broad spectrum of important new achievements in the field of artificial organs, ranging from fundamental research to clinical applications. The scope of the Journal of Artificial Organs encompasses but is not restricted to blood purification, cardiovascular intervention, biomaterials, and artificial metabolic organs. Additionally, the journal will cover technical and industrial innovations. Membership in the Japanese Society for Artificial Organs is not a prerequisite for submission.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


