Mustafa Al-Gburi, Ali Al-Hamdani, Jeppe Vejlgaard Rasmussen, Bo Sanderhoff Olsen
{"title":"Low risk of postoperative ulnar nerve affection in surgically treated distal humeral fractures when the nerve is released <i>in situ</i>.","authors":"Mustafa Al-Gburi, Ali Al-Hamdani, Jeppe Vejlgaard Rasmussen, Bo Sanderhoff Olsen","doi":"10.5312/wjo.v14.i7.526","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adult distal humeral fractures (DHF) comprise 2%-5% of all fractures and 30% of all elbow fractures. Treatment of DHF may be technically demanding due to fracture complexity and proximity of neurovascular structures. Open reduction and internal fixation (ORIF) are often the treatment of choice, but arthroplasty is considered in case of severe comminution or in elderly patients with poor bone quality. Ulnar nerve affection following surgical treatment of distal humerus fractures is a well-recognized complication.</p><p><strong>Aim: </strong>To report the risk of ulnar nerve affection after surgery for acute DHFs.</p><p><strong>Methods: </strong>We retrospectively identified 239 consecutive adult patients with acute DHFs who underwent surgery with ORIF, elbow hemiarthroplasty (EHA) or total elbow arthroplasty (TEA) between January 2011 and December 2019. In all cases, the ulnar nerve was released <i>in situ</i> without anterior transposition. We used our institutional database to review patients' medical records for demographics, fracture morphology, type of surgery and ulnar nerve affection immediately; records were reviewed after surgery and at 2 wk and 12 wk of routine clinical outpatient follow-up. Twenty-nine percent patients were excluded due to pre- or postoperative conditions. Final follow-up examination was a telephone interview in which ulnar nerve affection was reported according to the McGowen Classification Score. A total of 210 patients were eligible for interview, but 13 patients declined participation and 17 patients failed to respond. Thus, 180 patients were included.</p><p><strong>Results: </strong>Mean age at surgery was 64 years (range 18-88 years); 121 (67.3%) patients were women; 59 (32.7%) were men. According to the AO/OTA classification system, we recorded 47 patients with type A3, 55 patients with type B and 78 patients with type C fractures. According to the McGowen Classification Score, mild ulnar nerve affection was reported in nine patients; severe affection, in two. A total of 69 patients were treated with ORIF of whom three had mild temporary ulnar nerve affection and one had severe ulnar nerve affection. In all, 111 patients were treated with arthroplasty (67 EHA, 44 TEA) of whom seven had mild ulnar nerve affection and one had severe persistent ulnar nerve affection. No further treatment was provided.</p><p><strong>Conclusion: </strong>The risk of ulnar nerve affection after surgical treatment for acute DHF is low when the ulnar nerve is released <i>in situ</i> without nerve transposition, independently of the treatment provided.</p>","PeriodicalId":47843,"journal":{"name":"World Journal of Orthopedics","volume":"14 7","pages":"526-532"},"PeriodicalIF":2.0000,"publicationDate":"2023-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/56/51/WJO-14-526.PMC10359752.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Orthopedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5312/wjo.v14.i7.526","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Adult distal humeral fractures (DHF) comprise 2%-5% of all fractures and 30% of all elbow fractures. Treatment of DHF may be technically demanding due to fracture complexity and proximity of neurovascular structures. Open reduction and internal fixation (ORIF) are often the treatment of choice, but arthroplasty is considered in case of severe comminution or in elderly patients with poor bone quality. Ulnar nerve affection following surgical treatment of distal humerus fractures is a well-recognized complication.
Aim: To report the risk of ulnar nerve affection after surgery for acute DHFs.
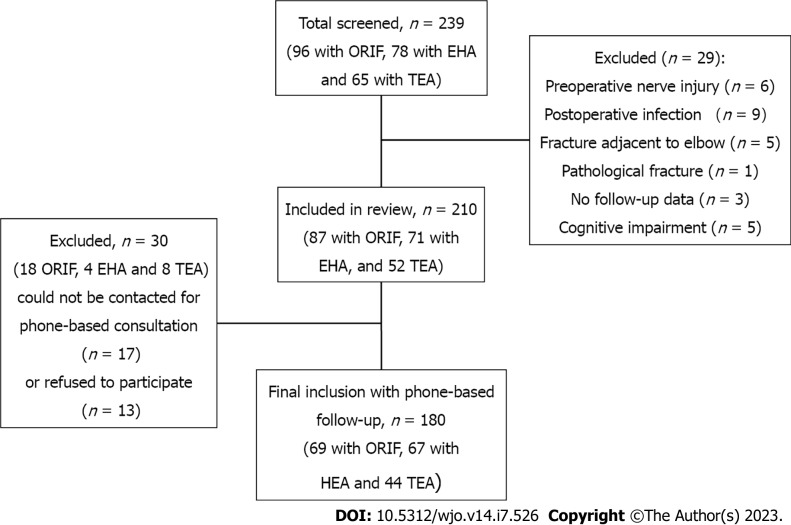
Methods: We retrospectively identified 239 consecutive adult patients with acute DHFs who underwent surgery with ORIF, elbow hemiarthroplasty (EHA) or total elbow arthroplasty (TEA) between January 2011 and December 2019. In all cases, the ulnar nerve was released in situ without anterior transposition. We used our institutional database to review patients' medical records for demographics, fracture morphology, type of surgery and ulnar nerve affection immediately; records were reviewed after surgery and at 2 wk and 12 wk of routine clinical outpatient follow-up. Twenty-nine percent patients were excluded due to pre- or postoperative conditions. Final follow-up examination was a telephone interview in which ulnar nerve affection was reported according to the McGowen Classification Score. A total of 210 patients were eligible for interview, but 13 patients declined participation and 17 patients failed to respond. Thus, 180 patients were included.
Results: Mean age at surgery was 64 years (range 18-88 years); 121 (67.3%) patients were women; 59 (32.7%) were men. According to the AO/OTA classification system, we recorded 47 patients with type A3, 55 patients with type B and 78 patients with type C fractures. According to the McGowen Classification Score, mild ulnar nerve affection was reported in nine patients; severe affection, in two. A total of 69 patients were treated with ORIF of whom three had mild temporary ulnar nerve affection and one had severe ulnar nerve affection. In all, 111 patients were treated with arthroplasty (67 EHA, 44 TEA) of whom seven had mild ulnar nerve affection and one had severe persistent ulnar nerve affection. No further treatment was provided.
Conclusion: The risk of ulnar nerve affection after surgical treatment for acute DHF is low when the ulnar nerve is released in situ without nerve transposition, independently of the treatment provided.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


