Wajiha Zahra, Mina Seifo, Paul Cool, David Ford, Tosan Okoro
{"title":"Clinical outcome of open ankle fractures in patients above 70 years of age.","authors":"Wajiha Zahra, Mina Seifo, Paul Cool, David Ford, Tosan Okoro","doi":"10.5312/wjo.v14.i7.554","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Open fractures of the ankle are complex injuries requiring multidisciplinary input and are associated with significant morbidity and mortality. However, data on the clinical outcomes of open ankle fracture management in patients older than 70 is minimal.</p><p><strong>Aim: </strong>To evaluate the clinical outcomes following open ankle fracture management in patients older than 70. Our secondary aim is to look at predictors of poor outcomes.</p><p><strong>Methods: </strong>Following local research and audit department registration, 22 years of prospectively collated data from an electronic database in a district general hospital were assessed. All patients older than 70 years of age with an open ankle fracture requiring surgical intervention were identified. Demographic information, the nature, and the number of surgical interventions were collated. Complications, including surgical site infection (SSI), venous thromboembolic events (VTEs) during hospital stay, and mortality rate, were reviewed.</p><p><strong>Results: </strong>A total of 37 patients were identified (median age: 84 years, range: 70-98); <i>n</i> = 30 females median age: 84 years, range: 70-97); <i>n</i> = 7 males median age: 74 years, range: 71-98)) who underwent surgical intervention after an open ankle fracture. Sixteen patients developed SSIs (43%). Superficial SSIs (<i>n</i> = 8) were managed without surgical intervention and treated with antibiotics and regular dressing changes. Deep SSIs (<i>n</i> = 8; 20%) required a median of 3 (range: 2-9) surgical interventions, with four patients requiring multiple washouts and one patient having metalwork removed. VTE incidence was 5% during the hospital stay. Eight patients died within 30 d, and mortality at one year was 19%. The 10-year mortality rate was 57%. The presence of a history of stroke, cancer, or prolonged inpatient stay was found to be predictive of lower survivorship in this population (log-rank test: cancer <i>P</i> = 0.008, stroke <i>P</i> = 0.001, length of stay > 33 d <i>P</i> = 0.015). The presence of a cardiac history was predictive of wound complications (logistic regression, <i>P</i> = 0.045). Age, number of operations, and diabetic history were found to be predictive of an increase in the length of stay (general linear model; age <i>P</i> < 0.001, number of operations <i>P</i> < 0.001, diabetes <i>P</i> = 0.041).</p><p><strong>Conclusion: </strong>An open ankle fracture in a patient older than 70 years has at least a 20% chance of requiring repeated surgical intervention due to deep SSIs. The presence of a cardiac history appears to be the main predictor for wound complications.</p>","PeriodicalId":47843,"journal":{"name":"World Journal of Orthopedics","volume":"14 7","pages":"554-561"},"PeriodicalIF":2.0000,"publicationDate":"2023-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6b/7d/WJO-14-554.PMC10359747.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Orthopedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5312/wjo.v14.i7.554","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Open fractures of the ankle are complex injuries requiring multidisciplinary input and are associated with significant morbidity and mortality. However, data on the clinical outcomes of open ankle fracture management in patients older than 70 is minimal.
Aim: To evaluate the clinical outcomes following open ankle fracture management in patients older than 70. Our secondary aim is to look at predictors of poor outcomes.
Methods: Following local research and audit department registration, 22 years of prospectively collated data from an electronic database in a district general hospital were assessed. All patients older than 70 years of age with an open ankle fracture requiring surgical intervention were identified. Demographic information, the nature, and the number of surgical interventions were collated. Complications, including surgical site infection (SSI), venous thromboembolic events (VTEs) during hospital stay, and mortality rate, were reviewed.
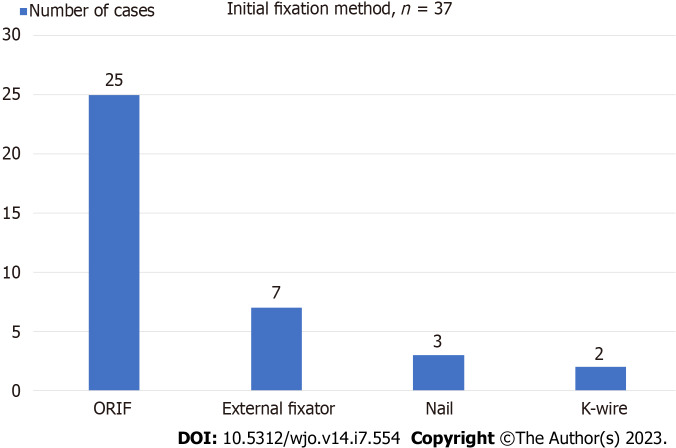
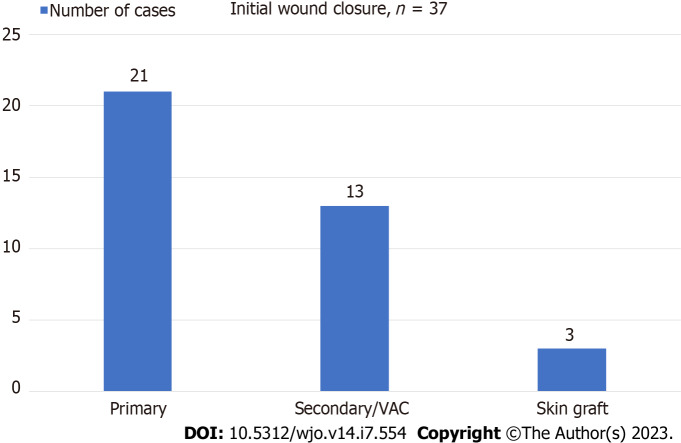
Results: A total of 37 patients were identified (median age: 84 years, range: 70-98); n = 30 females median age: 84 years, range: 70-97); n = 7 males median age: 74 years, range: 71-98)) who underwent surgical intervention after an open ankle fracture. Sixteen patients developed SSIs (43%). Superficial SSIs (n = 8) were managed without surgical intervention and treated with antibiotics and regular dressing changes. Deep SSIs (n = 8; 20%) required a median of 3 (range: 2-9) surgical interventions, with four patients requiring multiple washouts and one patient having metalwork removed. VTE incidence was 5% during the hospital stay. Eight patients died within 30 d, and mortality at one year was 19%. The 10-year mortality rate was 57%. The presence of a history of stroke, cancer, or prolonged inpatient stay was found to be predictive of lower survivorship in this population (log-rank test: cancer P = 0.008, stroke P = 0.001, length of stay > 33 d P = 0.015). The presence of a cardiac history was predictive of wound complications (logistic regression, P = 0.045). Age, number of operations, and diabetic history were found to be predictive of an increase in the length of stay (general linear model; age P < 0.001, number of operations P < 0.001, diabetes P = 0.041).
Conclusion: An open ankle fracture in a patient older than 70 years has at least a 20% chance of requiring repeated surgical intervention due to deep SSIs. The presence of a cardiac history appears to be the main predictor for wound complications.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


