{"title":"Symptomatologic pathomechanism of <i>N</i>-methyl D-aspartate receptor encephalitis.","authors":"Woo-Jin Lee","doi":"10.47936/encephalitis.2021.00017","DOIUrl":null,"url":null,"abstract":"<p><p><i>N</i>-methyl D-aspartate receptor (NMDAR) encephalitis is a well-characterized clinical syndrome. The main molecular mechanism of NMDAR encephalitis is autoantibody-mediated NMDAR hypofunction in the neuronal synapse. Several pathomechanistic hypotheses might explain how NMDAR hypofunction causes the typical symptoms and prognosis of NMDAR encephalitis. Suppression of NMDAR-dependent gamma-aminobutyric acid interneurons provokes an accelerated activation of the positive feedback loops of the dorsolateral prefrontal cortex/subiculum-nucleus accumbens circuit in the striatum, the ventral tegmental area (VTA), and the nucleus reuniens in the thalamus-hippocampus-VTA loop. Dysregulated activation of the VTA and cortex via those positive feedback loops may explain the rapid clinical deterioration at acute stages of the disease and the well-characterized syndrome that includes limbic system dysfunction, intractable seizures, dyskinesia, coma, and the characteristic extreme delta brush. Progressive cerebellar atrophy is correlated with cumulative disease burden and is associated with worse long-term outcomes, which might be explained by the NMDAR-dependent pathways required to maintain neuronal survival. Those pathomechanistic hypotheses for NMDAR encephalitis support the rationale for the early introduction of combination immunotherapy and the use of adjuvant immunotherapy in patients with persisting symptoms in chronic disease phases.</p>","PeriodicalId":72904,"journal":{"name":"Encephalitis (Seoul, Korea)","volume":"1 2","pages":"36-44"},"PeriodicalIF":0.0000,"publicationDate":"2021-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/51/e6/encephalitis-2021-00017.PMC10295887.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Encephalitis (Seoul, Korea)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.47936/encephalitis.2021.00017","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
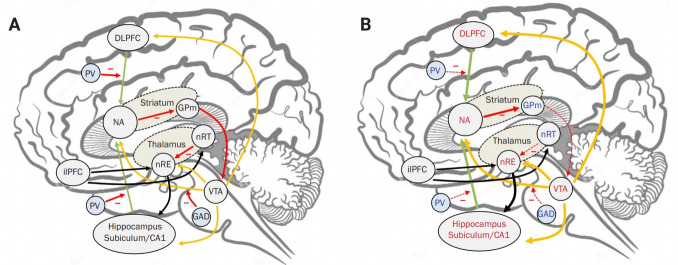
N-methyl D-aspartate receptor (NMDAR) encephalitis is a well-characterized clinical syndrome. The main molecular mechanism of NMDAR encephalitis is autoantibody-mediated NMDAR hypofunction in the neuronal synapse. Several pathomechanistic hypotheses might explain how NMDAR hypofunction causes the typical symptoms and prognosis of NMDAR encephalitis. Suppression of NMDAR-dependent gamma-aminobutyric acid interneurons provokes an accelerated activation of the positive feedback loops of the dorsolateral prefrontal cortex/subiculum-nucleus accumbens circuit in the striatum, the ventral tegmental area (VTA), and the nucleus reuniens in the thalamus-hippocampus-VTA loop. Dysregulated activation of the VTA and cortex via those positive feedback loops may explain the rapid clinical deterioration at acute stages of the disease and the well-characterized syndrome that includes limbic system dysfunction, intractable seizures, dyskinesia, coma, and the characteristic extreme delta brush. Progressive cerebellar atrophy is correlated with cumulative disease burden and is associated with worse long-term outcomes, which might be explained by the NMDAR-dependent pathways required to maintain neuronal survival. Those pathomechanistic hypotheses for NMDAR encephalitis support the rationale for the early introduction of combination immunotherapy and the use of adjuvant immunotherapy in patients with persisting symptoms in chronic disease phases.
n -甲基d -天冬氨酸受体(NMDAR)脑炎是一种典型的临床综合征。NMDAR脑炎的主要分子机制是自身抗体介导的神经元突触NMDAR功能减退。几种病理机制假说可以解释NMDAR功能减退如何导致NMDAR脑炎的典型症状和预后。抑制nmdar依赖的γ -氨基丁酸中间神经元会加速激活纹状体背外侧前额叶皮层/丘下-伏隔核回路、腹侧被盖区(VTA)和丘脑-海马-VTA回路中的联合核的正反馈回路。通过这些正反馈回路的VTA和皮层的失调激活可能解释了疾病急性阶段的快速临床恶化和典型的综合征,包括边缘系统功能障碍、难治性癫痫、运动障碍、昏迷和特征性的极端三角刷。进行性小脑萎缩与累积性疾病负担相关,并与较差的长期预后相关,这可能与维持神经元存活所需的nmdar依赖通路有关。这些NMDAR脑炎的病理机制假说支持了早期引入联合免疫治疗和在慢性病期持续症状患者中使用辅助免疫治疗的基本原理。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


