Transjugular Intrahepatic Portosystemic Shunt With or Without Gastroesophageal Variceal Embolization for the Prevention of Variceal Rebleeding: A Systematic Review and Meta-Analysis.
Fouad Jaber, Azizullah Beran, Saqr Alsakarneh, Khalid Ahmed, Mohamed Abdallah, Khaled Elfert, Mohammad Almeqdadi, Mohammed Jaber, Wael T Mohamed, Mohamd Ahmed, Laith Al Momani, Laith Numan, Thomas Bierman, John H Helzberg, Hassan Ghoz, Wendell K Clarkston
{"title":"Transjugular Intrahepatic Portosystemic Shunt With or Without Gastroesophageal Variceal Embolization for the Prevention of Variceal Rebleeding: A Systematic Review and Meta-Analysis.","authors":"Fouad Jaber, Azizullah Beran, Saqr Alsakarneh, Khalid Ahmed, Mohamed Abdallah, Khaled Elfert, Mohammad Almeqdadi, Mohammed Jaber, Wael T Mohamed, Mohamd Ahmed, Laith Al Momani, Laith Numan, Thomas Bierman, John H Helzberg, Hassan Ghoz, Wendell K Clarkston","doi":"10.14740/gr1618","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The role of variceal embolization (VE) during transjugular intrahepatic portosystemic shunt (TIPS) creation for preventing gastroesophageal variceal rebleeding remains controversial. Therefore, we performed a meta-analysis to compare the incidence of variceal rebleeding, shunt dysfunction, encephalopathy, and death between patients treated with TIPS alone and those treated with TIPS in combination with VE.</p><p><strong>Methods: </strong>We performed a literature search using PubMed, EMBASE, Scopus, and Cochrane databases for all studies comparing the incidence of complications between TIPS alone and TIPS with VE. The primary outcome was variceal rebleeding. Secondary outcomes include shunt dysfunction, encephalopathy, and death. Subgroup analysis was performed based on the type of stent (covered vs. bare metal). The random-effects model was used to calculate the relative risk (RR) with the corresponding 95% confidence intervals (CIs) of outcome. A P value < 0.05 was considered statistically significant.</p><p><strong>Results: </strong>Eleven studies with a total of 1,075 patients were included (597: TIPS alone and 478: TIPS plus VE). Compared to the TIPS alone, the TIPS with VE had a significantly lower incidence of variceal rebleeding (RR: 0.59, 95% CI: 0.43 - 0.81, P = 0.001). Subgroup analysis revealed similar results in covered stents (RR: 0.56, 95% CI: 0.36 - 0.86, P = 0.008) but there was no significant difference between the two groups in the subgroup analysis of bare stents and combined stents. There was no significant difference in the risk of encephalopathy (RR: 0.84, 95% CI: 0.66 - 1.06, P = 0.13), shunt dysfunction (RR: 0.88, 95% CI: 0.64 - 1.19, P = 0.40), and death (RR: 0.87, 95% CI: 0.65 - 1.17, P = 0.34). There were similarly no differences in these secondary outcomes between groups when stratified according to type of stent.</p><p><strong>Conclusions: </strong>Adding VE to TIPS reduced the incidence of variceal rebleeding in patients with cirrhosis. However, the benefit was observed with covered stents only. Further large-scale randomized controlled trials are warranted to validate our findings.</p>","PeriodicalId":12461,"journal":{"name":"Gastroenterology Research","volume":"16 2","pages":"68-78"},"PeriodicalIF":1.7000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a0/42/gr-16-068.PMC10181335.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastroenterology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/gr1618","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The role of variceal embolization (VE) during transjugular intrahepatic portosystemic shunt (TIPS) creation for preventing gastroesophageal variceal rebleeding remains controversial. Therefore, we performed a meta-analysis to compare the incidence of variceal rebleeding, shunt dysfunction, encephalopathy, and death between patients treated with TIPS alone and those treated with TIPS in combination with VE.
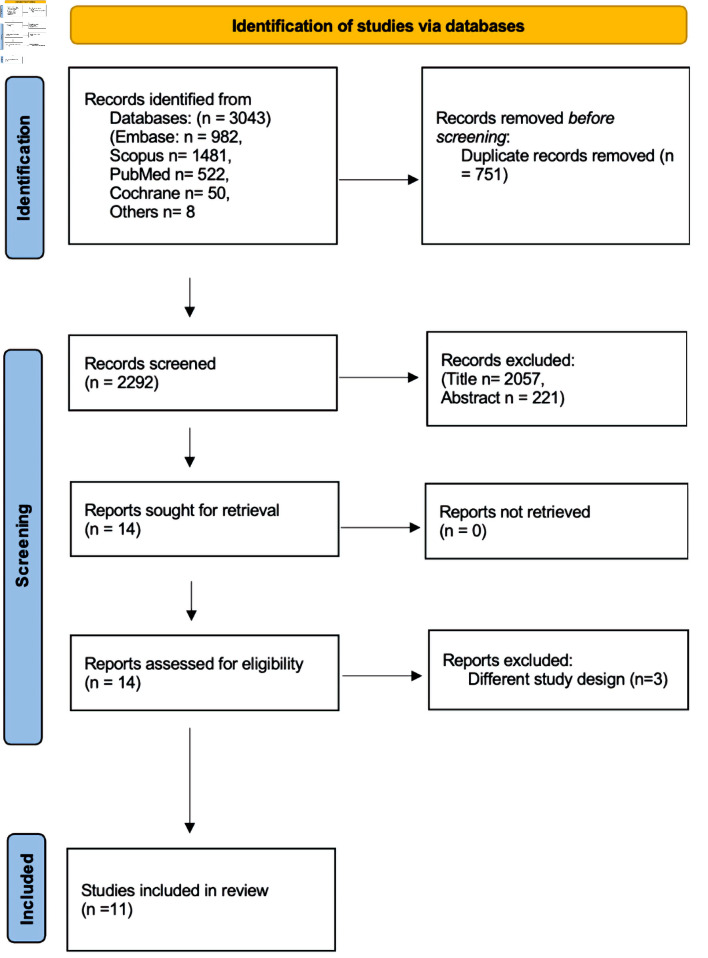
Methods: We performed a literature search using PubMed, EMBASE, Scopus, and Cochrane databases for all studies comparing the incidence of complications between TIPS alone and TIPS with VE. The primary outcome was variceal rebleeding. Secondary outcomes include shunt dysfunction, encephalopathy, and death. Subgroup analysis was performed based on the type of stent (covered vs. bare metal). The random-effects model was used to calculate the relative risk (RR) with the corresponding 95% confidence intervals (CIs) of outcome. A P value < 0.05 was considered statistically significant.
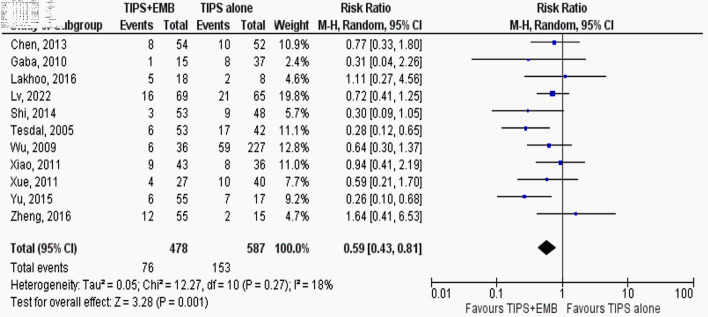
Results: Eleven studies with a total of 1,075 patients were included (597: TIPS alone and 478: TIPS plus VE). Compared to the TIPS alone, the TIPS with VE had a significantly lower incidence of variceal rebleeding (RR: 0.59, 95% CI: 0.43 - 0.81, P = 0.001). Subgroup analysis revealed similar results in covered stents (RR: 0.56, 95% CI: 0.36 - 0.86, P = 0.008) but there was no significant difference between the two groups in the subgroup analysis of bare stents and combined stents. There was no significant difference in the risk of encephalopathy (RR: 0.84, 95% CI: 0.66 - 1.06, P = 0.13), shunt dysfunction (RR: 0.88, 95% CI: 0.64 - 1.19, P = 0.40), and death (RR: 0.87, 95% CI: 0.65 - 1.17, P = 0.34). There were similarly no differences in these secondary outcomes between groups when stratified according to type of stent.
Conclusions: Adding VE to TIPS reduced the incidence of variceal rebleeding in patients with cirrhosis. However, the benefit was observed with covered stents only. Further large-scale randomized controlled trials are warranted to validate our findings.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


