Fabrizio Ceresa, Aurora Leonardi, Filomena Bruna De Donno, Auguto Palermo, Liborio Francesco Mammana, Francesco Patanè
{"title":"Left Atrial Appendage Closure Device Embolization under the Anterior Leaflet of Mitral Valve: Echocardiographic Diagnosis and Management.","authors":"Fabrizio Ceresa, Aurora Leonardi, Filomena Bruna De Donno, Auguto Palermo, Liborio Francesco Mammana, Francesco Patanè","doi":"10.4103/jcecho.jcecho_56_22","DOIUrl":null,"url":null,"abstract":"<p><p>A 76-year-old man with history of previous coronary artery bypass grafting, permanent atrial fibrillation in novel oral anticoagulation therapy, and gastrointestinal bleedings underwent percutaneous left atrial appendage closure. The procedure was complicated by intraoperative device embolization, which caused a dynamic obstruction of the left ventricular outflow tract leading to severe hemodynamic instability. Transesophageal echocardiography showed a device in the ventricle site of the mitral anterior leaflet. The coronary angiography showed also patency of both arterial grafts in stable coronary artery disease. After failing the percutaneous retrieval with a snare, emergent surgery was planned. A moderate calcified aortic valve stenosis was also found, but in consideration of the unstable clinical conditions of the patient, we thought of performing a transcatheter aortic valve replacement (TAVR) in a second time. We have carefully planned the surgical retrieval of the device embolized paying attention of his several comorbidities. The strategy to remove the device with cardiopulmonary bypass without cross-clamping the aorta through a right mini-thoracotomy has been preferred.</p>","PeriodicalId":15191,"journal":{"name":"Journal of Cardiovascular Echography","volume":"33 1","pages":"40-42"},"PeriodicalIF":1.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10328133/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Echography","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcecho.jcecho_56_22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/5/29 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
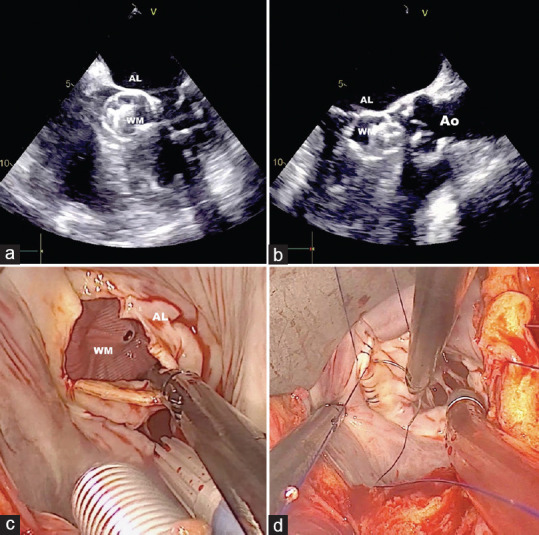
A 76-year-old man with history of previous coronary artery bypass grafting, permanent atrial fibrillation in novel oral anticoagulation therapy, and gastrointestinal bleedings underwent percutaneous left atrial appendage closure. The procedure was complicated by intraoperative device embolization, which caused a dynamic obstruction of the left ventricular outflow tract leading to severe hemodynamic instability. Transesophageal echocardiography showed a device in the ventricle site of the mitral anterior leaflet. The coronary angiography showed also patency of both arterial grafts in stable coronary artery disease. After failing the percutaneous retrieval with a snare, emergent surgery was planned. A moderate calcified aortic valve stenosis was also found, but in consideration of the unstable clinical conditions of the patient, we thought of performing a transcatheter aortic valve replacement (TAVR) in a second time. We have carefully planned the surgical retrieval of the device embolized paying attention of his several comorbidities. The strategy to remove the device with cardiopulmonary bypass without cross-clamping the aorta through a right mini-thoracotomy has been preferred.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


