{"title":"Low Accuracy of Antenatal Screening for Group B Streptococcus From Perianal Area.","authors":"Shunji Suzuki","doi":"10.14740/jocmr4927","DOIUrl":null,"url":null,"abstract":"Group B streptococcus (GBS) is recognized as the most frequent cause of severe early-onset infection in newborn infants. GBS has been observed to be present in the bowel flora of 17.4% of adults (colonization) including pregnant women, and those who are colonized are called “carriers” [1]. To date, more than half of early-onset GBS disease has been reported to occur in neonates born to women with negative GBS screening tests [2, 3]. For example, the recent article in Japan by Miyata et al [2] has also concerned that early-onset GBS disease can develop in infants who are born to mothers with negative GBS screening results. The timing of GBS screening at 35 37 weeks recommended by the Centers for Disease Control and Prevention (CDC) [4] and the American College of Obstetricians and Gynecologists (ACOG) [5] was established based on an earlier study by Yancey et al [6], which indicated that the accuracy of late antenatal anogenital cultures in predicting GBS colonization at delivery is high in cultures collected at 1 5 weeks before delivery. In their observation, the sensitivity, specificity, positive predictive value, and negative predictive value of GBS cultures at 1 5 weeks before delivery for identifying colonization status at delivery were 87%, 96%, 87%, and 96%, respectively. While they were only 43%, 85%, 50%, and 81%, respectively among patients cultured 6 or more weeks before delivery. In their observation [6], a swab for culture specimen was inserted through the anal sphincter; however, the vaginal-perianal collection method has been indicated to be less painful and comfortable [7]. In some recent examinations [7-9], the detection rates of GBS culture from the (vaginal-) perianal area have been observed to be similar to that of anorectal specimens; however, the accuracy of antenatal screening for GBS with cultures from the perianal area has not been well examined. The protocol for this prospective study was approved by the Ethics Committee of Japanese Red Cross Katsushika Maternity Hospital (K2007-15). Informed consent concerning analysis was obtained from all subjects. We performed maternal GBS culture from perianal area used non-selective enrichment medium in 93 Japanese pregnant women scheduled vaginal delivery with GBS-positive at 35 weeks’ gestation every week until delivery. Of these, 84 (90%) delivered at ≤ 40 weeks’ gestation (within 5 weeks). The clinical characteristics of the 84 women are shown in Table 1. All women received the administration of ampicillin intravenous (IV) during labor or after premature membrane rupture. Fortunately, there were no cases of neonatal infection as shown in Table 1. At 36 weeks’ gestation, 62 of these were defined as GBSpositive (positive predictive value: 74%), while 22 (26%) were negative. At 37 weeks’ gestation, the different results from those of the previous week (36 weeks’ gestation) were defined in 29 (15 + 14: 35%) women as shown in Figure 1. At the last perinatal visits, GBS-positive was defined in only 60 women (71%). In this study, the reproducibility rate of GBS-positive at perianal area within 5 weeks was only 71-74%. It seemed to be lower than that at anorectal area (inner part of anal sphincter) (87%) as previously reported [6]. Although the detection rates of GBS culture from perianal area may be similar to that from anorectal area [7-9]; however, the accuracy of antenatal screening for GBS with cultures from the perianal area may be inferior to that from anorectal area. The low accuracy in GBS colonization cultured from perianal area may be influenced by the status of defecation and rear cleaning. There may also be the influence of urination and shower bath before examination. On the other hand, there may be women diagnosed as GBS-negative accidentally at 35 weeks’ gestation. We understand that the use of non-selective medium is one of the limitations in this study, because GBS selectivity may be reduced by the overgrowth of other bacterial species other than GBS during the culture process [10]. How-","PeriodicalId":15431,"journal":{"name":"Journal of Clinical Medicine Research","volume":"15 6","pages":"340-342"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/66/05/jocmr-15-340.PMC10332875.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Medicine Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr4927","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
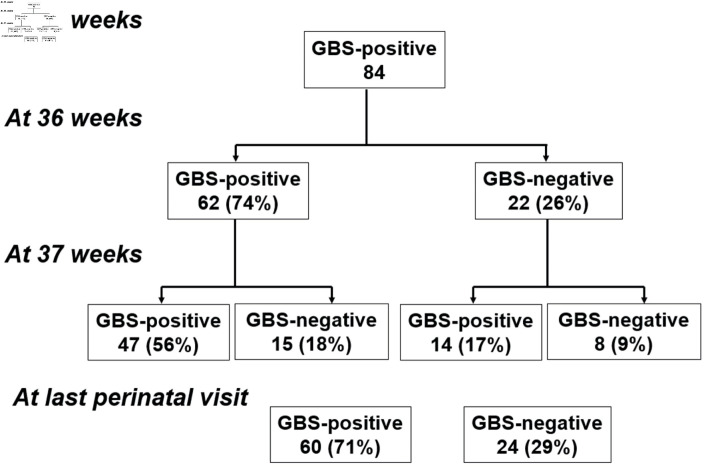
Group B streptococcus (GBS) is recognized as the most frequent cause of severe early-onset infection in newborn infants. GBS has been observed to be present in the bowel flora of 17.4% of adults (colonization) including pregnant women, and those who are colonized are called “carriers” [1]. To date, more than half of early-onset GBS disease has been reported to occur in neonates born to women with negative GBS screening tests [2, 3]. For example, the recent article in Japan by Miyata et al [2] has also concerned that early-onset GBS disease can develop in infants who are born to mothers with negative GBS screening results. The timing of GBS screening at 35 37 weeks recommended by the Centers for Disease Control and Prevention (CDC) [4] and the American College of Obstetricians and Gynecologists (ACOG) [5] was established based on an earlier study by Yancey et al [6], which indicated that the accuracy of late antenatal anogenital cultures in predicting GBS colonization at delivery is high in cultures collected at 1 5 weeks before delivery. In their observation, the sensitivity, specificity, positive predictive value, and negative predictive value of GBS cultures at 1 5 weeks before delivery for identifying colonization status at delivery were 87%, 96%, 87%, and 96%, respectively. While they were only 43%, 85%, 50%, and 81%, respectively among patients cultured 6 or more weeks before delivery. In their observation [6], a swab for culture specimen was inserted through the anal sphincter; however, the vaginal-perianal collection method has been indicated to be less painful and comfortable [7]. In some recent examinations [7-9], the detection rates of GBS culture from the (vaginal-) perianal area have been observed to be similar to that of anorectal specimens; however, the accuracy of antenatal screening for GBS with cultures from the perianal area has not been well examined. The protocol for this prospective study was approved by the Ethics Committee of Japanese Red Cross Katsushika Maternity Hospital (K2007-15). Informed consent concerning analysis was obtained from all subjects. We performed maternal GBS culture from perianal area used non-selective enrichment medium in 93 Japanese pregnant women scheduled vaginal delivery with GBS-positive at 35 weeks’ gestation every week until delivery. Of these, 84 (90%) delivered at ≤ 40 weeks’ gestation (within 5 weeks). The clinical characteristics of the 84 women are shown in Table 1. All women received the administration of ampicillin intravenous (IV) during labor or after premature membrane rupture. Fortunately, there were no cases of neonatal infection as shown in Table 1. At 36 weeks’ gestation, 62 of these were defined as GBSpositive (positive predictive value: 74%), while 22 (26%) were negative. At 37 weeks’ gestation, the different results from those of the previous week (36 weeks’ gestation) were defined in 29 (15 + 14: 35%) women as shown in Figure 1. At the last perinatal visits, GBS-positive was defined in only 60 women (71%). In this study, the reproducibility rate of GBS-positive at perianal area within 5 weeks was only 71-74%. It seemed to be lower than that at anorectal area (inner part of anal sphincter) (87%) as previously reported [6]. Although the detection rates of GBS culture from perianal area may be similar to that from anorectal area [7-9]; however, the accuracy of antenatal screening for GBS with cultures from the perianal area may be inferior to that from anorectal area. The low accuracy in GBS colonization cultured from perianal area may be influenced by the status of defecation and rear cleaning. There may also be the influence of urination and shower bath before examination. On the other hand, there may be women diagnosed as GBS-negative accidentally at 35 weeks’ gestation. We understand that the use of non-selective medium is one of the limitations in this study, because GBS selectivity may be reduced by the overgrowth of other bacterial species other than GBS during the culture process [10]. How-

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


