Ashley B Brown, Charles Miller, Davidson H Hamer, Phyllis Kozarsky, Michael Libman, Ralph Huits, Aisha Rizwan, Hannah Emetulu, Jesse Waggoner, Lin H Chen, Daniel T Leung, Daniel Bourque, Bradley A Connor, Carmelo Licitra, Kristina M Angelo
{"title":"Travel-Related Diagnoses Among U.S. Nonmigrant Travelers or Migrants Presenting to U.S. GeoSentinel Sites - GeoSentinel Network, 2012-2021.","authors":"Ashley B Brown, Charles Miller, Davidson H Hamer, Phyllis Kozarsky, Michael Libman, Ralph Huits, Aisha Rizwan, Hannah Emetulu, Jesse Waggoner, Lin H Chen, Daniel T Leung, Daniel Bourque, Bradley A Connor, Carmelo Licitra, Kristina M Angelo","doi":"10.15585/mmwr.ss7207a1","DOIUrl":null,"url":null,"abstract":"<p><strong>Problem/condition: </strong>During 2012-2021, the volume of international travel reached record highs and lows. This period also was marked by the emergence or large outbreaks of multiple infectious diseases (e.g., Zika virus, yellow fever, and COVID-19). Over time, the growing ease and increased frequency of travel has resulted in the unprecedented global spread of infectious diseases. Detecting infectious diseases and other diagnoses among travelers can serve as sentinel surveillance for new or emerging pathogens and provide information to improve case identification, clinical management, and public health prevention and response.</p><p><strong>Reporting period: </strong>2012-2021.</p><p><strong>Description of system: </strong>Established in 1995, the GeoSentinel Network (GeoSentinel), a collaboration between CDC and the International Society of Travel Medicine, is a global, clinical-care-based surveillance and research network of travel and tropical medicine sites that monitors infectious diseases and other adverse health events that affect international travelers. GeoSentinel comprises 71 sites in 29 countries where clinicians diagnose illnesses and collect demographic, clinical, and travel-related information about diseases and illnesses acquired during travel using a standardized report form. Data are collected electronically via a secure CDC database, and daily reports are generated for assistance in detecting sentinel events (i.e., unusual patterns or clusters of disease). GeoSentinel sites collaborate to report disease or population-specific findings through retrospective database analyses and the collection of supplemental data to fill specific knowledge gaps. GeoSentinel also serves as a communications network by using internal notifications, ProMed alerts, and peer-reviewed publications to alert clinicians and public health professionals about global outbreaks and events that might affect travelers. This report summarizes data from 20 U.S. GeoSentinel sites and reports on the detection of three worldwide events that demonstrate GeoSentinel's notification capability.</p><p><strong>Results: </strong>During 2012-2021, data were collected by all GeoSentinel sites on approximately 200,000 patients who had approximately 244,000 confirmed or probable travel-related diagnoses. Twenty GeoSentinel sites from the United States contributed records during the 10-year surveillance period, submitting data on 18,336 patients, of which 17,389 lived in the United States and were evaluated by a clinician at a U.S. site after travel. Of those patients, 7,530 (43.3%) were recent migrants to the United States, and 9,859 (56.7%) were returning nonmigrant travelers.Among the recent migrants to the United States, the median age was 28.5 years (range = <19 years to 93 years); 47.3% were female, and 6.0% were U.S. citizens. A majority (89.8%) were seen as outpatients, and among 4,672 migrants with information available, 4,148 (88.8%) did not receive pretravel health information. Of 13,986 diagnoses among migrants, the most frequent were vitamin D deficiency (20.2%), Blastocystis (10.9%), and latent tuberculosis (10.3%). Malaria was diagnosed in 54 (<1%) migrants. Of the 26 migrants diagnosed with malaria for whom pretravel information was known, 88.5% did not receive pretravel health information. Before November 16, 2018, patients' reasons for travel, exposure country, and exposure region were not linked to an individual diagnosis. Thus, results of these data from January 1, 2012, to November 15, 2018 (early period), and from November 16, 2018, to December 31, 2021 (later period), are reported separately. During the early and later periods, the most frequent regions of exposure were Sub-Saharan Africa (22.7% and 26.2%, respectively), the Caribbean (21.3% and 8.4%, respectively), Central America (13.4% and 27.6%, respectively), and South East Asia (13.1% and 16.9%, respectively). Migrants with diagnosed malaria were most frequently exposed in Sub-Saharan Africa (89.3% and 100%, respectively).Among nonmigrant travelers returning to the United States, the median age was 37 years (range = <19 years to 96 years); 55.7% were female, 75.3% were born in the United States, and 89.4% were U.S. citizens. A majority (90.6%) were seen as outpatients, and of 8,967 nonmigrant travelers with available information, 5,878 (65.6%) did not receive pretravel health information. Of 11,987 diagnoses, the most frequent were related to the gastrointestinal system (5,173; 43.2%). The most frequent diagnoses among nonmigrant travelers were acute diarrhea (16.9%), viral syndrome (4.9%), and irritable bowel syndrome (4.1%).Malaria was diagnosed in 421 (3.5%) nonmigrant travelers. During the early (January 1, 2012, to November 15, 2018) and later (November 16, 2018, to December 31, 2021) periods, the most frequent reasons for travel among nonmigrant travelers were tourism (44.8% and 53.6%, respectively), travelers visiting friends and relatives (VFRs) (22.0% and 21.4%, respectively), business (13.4% and 12.3%, respectively), and missionary or humanitarian aid (13.1% and 6.2%, respectively). The most frequent regions of exposure for any diagnosis among nonmigrant travelers during the early and later period were Central America (19.2% and 17.3%, respectively), Sub-Saharan Africa (17.7% and 25.5%, respectively), the Caribbean (13.0% and 10.9%, respectively), and South East Asia (10.4% and 11.2%, respectively).Nonmigrant travelers who had malaria diagnosed were most frequently exposed in Sub-Saharan Africa (88.6% and 95.9% during the early and later period, respectively) and VFRs (70.3% and 57.9%, respectively). Among VFRs with malaria, a majority did not receive pretravel health information (70.2% and 83.3%, respectively) or take malaria chemoprophylaxis (88.3% and 100%, respectively).</p><p><strong>Interpretation: </strong>Among ill U.S. travelers evaluated at U.S. GeoSentinel sites after travel, the majority were nonmigrant travelers who most frequently received a gastrointestinal disease diagnosis, implying that persons from the United States traveling internationally might be exposed to contaminated food and water. Migrants most frequently received diagnoses of conditions such as vitamin D deficiency and latent tuberculosis, which might result from adverse circumstances before and during migration (e.g., malnutrition and food insecurity, limited access to adequate sanitation and hygiene, and crowded housing,). Malaria was diagnosed in both migrants and nonmigrant travelers, and only a limited number reported taking malaria chemoprophylaxis, which might be attributed to both barriers to acquiring pretravel health care (especially for VFRs) and lack of prevention practices (e.g., insect repellant use) during travel. The number of ill travelers evaluated by U.S. GeoSentinel sites after travel decreased in 2020 and 2021 compared with previous years because of the COVID-19 pandemic and associated travel restrictions. GeoSentinel detected limited cases of COVID-19 and did not detect any sentinel cases early in the pandemic because of the lack of global diagnostic testing capacity.</p><p><strong>Public health action: </strong>The findings in this report describe the scope of health-related conditions that migrants and returning nonmigrant travelers to the United States acquired, illustrating risk for acquiring illnesses during travel. In addition, certain travelers do not seek pretravel health care, even when traveling to areas in which high-risk, preventable diseases are endemic. Health care professionals can aid international travelers by providing evaluations and destination-specific advice.Health care professionals should both foster trust and enhance pretravel prevention messaging for VFRs, a group known to have a higher incidence of serious diseases after travel (e.g., malaria and enteric fever). Health care professionals should continue to advocate for medical care in underserved populations (e.g., VFRs and migrants) to prevent disease progression, reactivation, and potential spread to and within vulnerable populations. Because both travel and infectious diseases evolve, public health professionals should explore ways to enhance the detection of emerging diseases that might not be captured by current surveillance systems that are not site based.</p>","PeriodicalId":48549,"journal":{"name":"Mmwr Surveillance Summaries","volume":"72 7","pages":"1-22"},"PeriodicalIF":37.3000,"publicationDate":"2023-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10332343/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mmwr Surveillance Summaries","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.15585/mmwr.ss7207a1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Problem/condition: During 2012-2021, the volume of international travel reached record highs and lows. This period also was marked by the emergence or large outbreaks of multiple infectious diseases (e.g., Zika virus, yellow fever, and COVID-19). Over time, the growing ease and increased frequency of travel has resulted in the unprecedented global spread of infectious diseases. Detecting infectious diseases and other diagnoses among travelers can serve as sentinel surveillance for new or emerging pathogens and provide information to improve case identification, clinical management, and public health prevention and response.
Reporting period: 2012-2021.
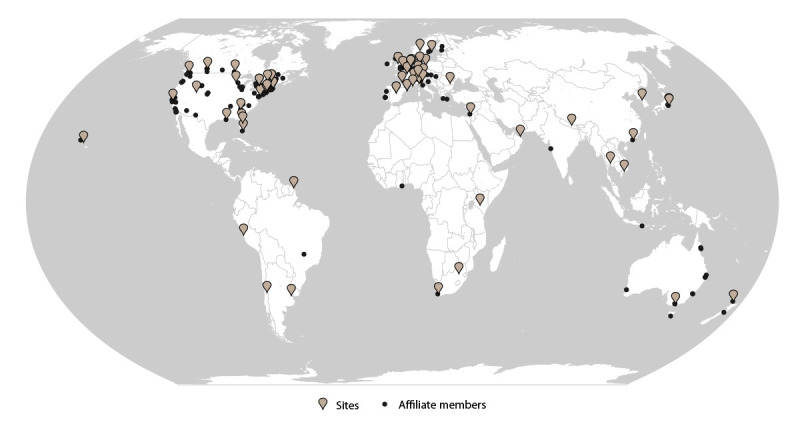
Description of system: Established in 1995, the GeoSentinel Network (GeoSentinel), a collaboration between CDC and the International Society of Travel Medicine, is a global, clinical-care-based surveillance and research network of travel and tropical medicine sites that monitors infectious diseases and other adverse health events that affect international travelers. GeoSentinel comprises 71 sites in 29 countries where clinicians diagnose illnesses and collect demographic, clinical, and travel-related information about diseases and illnesses acquired during travel using a standardized report form. Data are collected electronically via a secure CDC database, and daily reports are generated for assistance in detecting sentinel events (i.e., unusual patterns or clusters of disease). GeoSentinel sites collaborate to report disease or population-specific findings through retrospective database analyses and the collection of supplemental data to fill specific knowledge gaps. GeoSentinel also serves as a communications network by using internal notifications, ProMed alerts, and peer-reviewed publications to alert clinicians and public health professionals about global outbreaks and events that might affect travelers. This report summarizes data from 20 U.S. GeoSentinel sites and reports on the detection of three worldwide events that demonstrate GeoSentinel's notification capability.
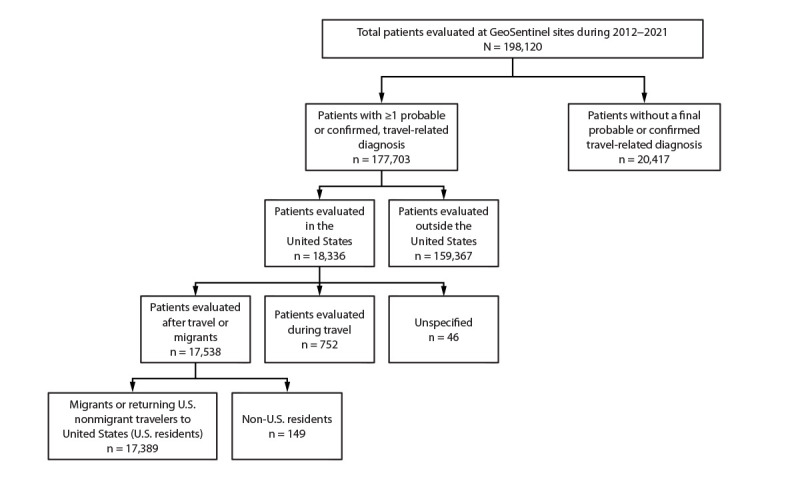
Results: During 2012-2021, data were collected by all GeoSentinel sites on approximately 200,000 patients who had approximately 244,000 confirmed or probable travel-related diagnoses. Twenty GeoSentinel sites from the United States contributed records during the 10-year surveillance period, submitting data on 18,336 patients, of which 17,389 lived in the United States and were evaluated by a clinician at a U.S. site after travel. Of those patients, 7,530 (43.3%) were recent migrants to the United States, and 9,859 (56.7%) were returning nonmigrant travelers.Among the recent migrants to the United States, the median age was 28.5 years (range = <19 years to 93 years); 47.3% were female, and 6.0% were U.S. citizens. A majority (89.8%) were seen as outpatients, and among 4,672 migrants with information available, 4,148 (88.8%) did not receive pretravel health information. Of 13,986 diagnoses among migrants, the most frequent were vitamin D deficiency (20.2%), Blastocystis (10.9%), and latent tuberculosis (10.3%). Malaria was diagnosed in 54 (<1%) migrants. Of the 26 migrants diagnosed with malaria for whom pretravel information was known, 88.5% did not receive pretravel health information. Before November 16, 2018, patients' reasons for travel, exposure country, and exposure region were not linked to an individual diagnosis. Thus, results of these data from January 1, 2012, to November 15, 2018 (early period), and from November 16, 2018, to December 31, 2021 (later period), are reported separately. During the early and later periods, the most frequent regions of exposure were Sub-Saharan Africa (22.7% and 26.2%, respectively), the Caribbean (21.3% and 8.4%, respectively), Central America (13.4% and 27.6%, respectively), and South East Asia (13.1% and 16.9%, respectively). Migrants with diagnosed malaria were most frequently exposed in Sub-Saharan Africa (89.3% and 100%, respectively).Among nonmigrant travelers returning to the United States, the median age was 37 years (range = <19 years to 96 years); 55.7% were female, 75.3% were born in the United States, and 89.4% were U.S. citizens. A majority (90.6%) were seen as outpatients, and of 8,967 nonmigrant travelers with available information, 5,878 (65.6%) did not receive pretravel health information. Of 11,987 diagnoses, the most frequent were related to the gastrointestinal system (5,173; 43.2%). The most frequent diagnoses among nonmigrant travelers were acute diarrhea (16.9%), viral syndrome (4.9%), and irritable bowel syndrome (4.1%).Malaria was diagnosed in 421 (3.5%) nonmigrant travelers. During the early (January 1, 2012, to November 15, 2018) and later (November 16, 2018, to December 31, 2021) periods, the most frequent reasons for travel among nonmigrant travelers were tourism (44.8% and 53.6%, respectively), travelers visiting friends and relatives (VFRs) (22.0% and 21.4%, respectively), business (13.4% and 12.3%, respectively), and missionary or humanitarian aid (13.1% and 6.2%, respectively). The most frequent regions of exposure for any diagnosis among nonmigrant travelers during the early and later period were Central America (19.2% and 17.3%, respectively), Sub-Saharan Africa (17.7% and 25.5%, respectively), the Caribbean (13.0% and 10.9%, respectively), and South East Asia (10.4% and 11.2%, respectively).Nonmigrant travelers who had malaria diagnosed were most frequently exposed in Sub-Saharan Africa (88.6% and 95.9% during the early and later period, respectively) and VFRs (70.3% and 57.9%, respectively). Among VFRs with malaria, a majority did not receive pretravel health information (70.2% and 83.3%, respectively) or take malaria chemoprophylaxis (88.3% and 100%, respectively).
Interpretation: Among ill U.S. travelers evaluated at U.S. GeoSentinel sites after travel, the majority were nonmigrant travelers who most frequently received a gastrointestinal disease diagnosis, implying that persons from the United States traveling internationally might be exposed to contaminated food and water. Migrants most frequently received diagnoses of conditions such as vitamin D deficiency and latent tuberculosis, which might result from adverse circumstances before and during migration (e.g., malnutrition and food insecurity, limited access to adequate sanitation and hygiene, and crowded housing,). Malaria was diagnosed in both migrants and nonmigrant travelers, and only a limited number reported taking malaria chemoprophylaxis, which might be attributed to both barriers to acquiring pretravel health care (especially for VFRs) and lack of prevention practices (e.g., insect repellant use) during travel. The number of ill travelers evaluated by U.S. GeoSentinel sites after travel decreased in 2020 and 2021 compared with previous years because of the COVID-19 pandemic and associated travel restrictions. GeoSentinel detected limited cases of COVID-19 and did not detect any sentinel cases early in the pandemic because of the lack of global diagnostic testing capacity.
Public health action: The findings in this report describe the scope of health-related conditions that migrants and returning nonmigrant travelers to the United States acquired, illustrating risk for acquiring illnesses during travel. In addition, certain travelers do not seek pretravel health care, even when traveling to areas in which high-risk, preventable diseases are endemic. Health care professionals can aid international travelers by providing evaluations and destination-specific advice.Health care professionals should both foster trust and enhance pretravel prevention messaging for VFRs, a group known to have a higher incidence of serious diseases after travel (e.g., malaria and enteric fever). Health care professionals should continue to advocate for medical care in underserved populations (e.g., VFRs and migrants) to prevent disease progression, reactivation, and potential spread to and within vulnerable populations. Because both travel and infectious diseases evolve, public health professionals should explore ways to enhance the detection of emerging diseases that might not be captured by current surveillance systems that are not site based.
期刊介绍:
The Morbidity and Mortality Weekly Report (MMWR) Series, produced by the Centers for Disease Control and Prevention (CDC), is commonly referred to as "the voice of CDC." Serving as the primary outlet for timely, reliable, authoritative, accurate, objective, and practical public health information and recommendations, the MMWR is a crucial publication. Its readership primarily includes physicians, nurses, public health practitioners, epidemiologists, scientists, researchers, educators, and laboratorians.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


