Hussam Jassim, Hassan A Nedaei, Ghazale Geraily, Nooshin Banaee, Ali Kazemian
{"title":"The geometric and dosimetric accuracy of kilovoltage cone beam computed tomography images for adaptive treatment: a systematic review.","authors":"Hussam Jassim, Hassan A Nedaei, Ghazale Geraily, Nooshin Banaee, Ali Kazemian","doi":"10.1259/bjro.20220062","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To provide an overview and meta-analysis of different techniques adopted to accomplish kVCBCT for dose calculation and automated segmentation.</p><p><strong>Methods: </strong>A systematic review and meta-analysis were performed on eligible studies demonstrating kVCBCT-based dose calculation and automated contouring of different tumor features. Meta-analysis of the performance was accomplished on the reported γ analysis and dice similarity coefficient (DSC) score of both collected results as three subgroups (head and neck, chest, and abdomen).</p><p><strong>Results: </strong>After the literature scrutinization (<i>n</i> = 1008), 52 papers were recognized for the systematic review. Nine studies of dosimtric studies and eleven studies of geometric analysis were suitable for inclusion in meta-analysis. Using kVCBCT for treatment replanning depends on a method used. Deformable Image Registration (DIR) methods yielded small dosimetric error (≤2%), γ pass rate (≥90%) and DSC (≥0.8). Hounsfield Unit (HU) override and calibration curve-based methods also achieved satisfactory yielded small dosimetric error (≤2%) and γ pass rate ((≥90%), but they are prone to error due to their sensitivity to a vendor-specific variation in kVCBCT image quality.</p><p><strong>Conclusions: </strong>Large cohorts of patients ought to be undertaken to validate methods achieving low levels of dosimetric and geometric errors. Quality guidelines should be established when reporting on kVCBCT, which include agreed metrics for reporting on the quality of corrected kVCBCT and defines protocols of new site-specific standardized imaging used when obtaining kVCBCT images for adaptive radiotherapy.</p><p><strong>Advances in knowledge: </strong>This review gives useful knowledge about methods making kVCBCT feasible for kVCBCT-based adaptive radiotherapy, simplifying patient pathway and reducing concomitant imaging dose to the patient.</p>","PeriodicalId":72419,"journal":{"name":"BJR open","volume":"5 1","pages":"20220062"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10301728/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJR open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1259/bjro.20220062","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Objectives: To provide an overview and meta-analysis of different techniques adopted to accomplish kVCBCT for dose calculation and automated segmentation.
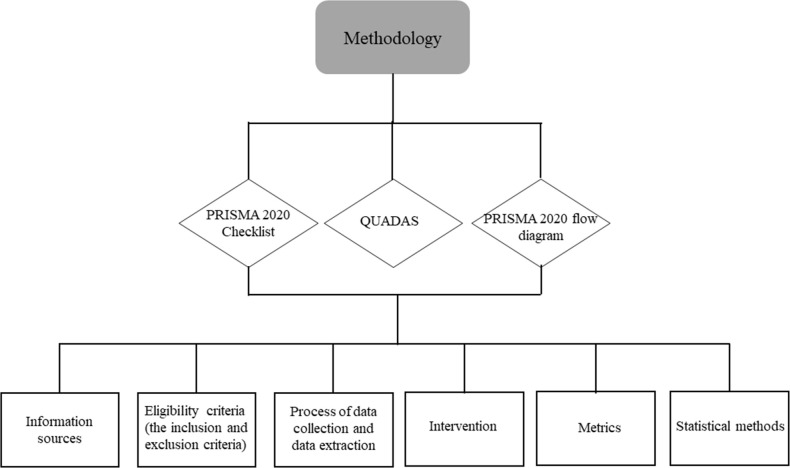
Methods: A systematic review and meta-analysis were performed on eligible studies demonstrating kVCBCT-based dose calculation and automated contouring of different tumor features. Meta-analysis of the performance was accomplished on the reported γ analysis and dice similarity coefficient (DSC) score of both collected results as three subgroups (head and neck, chest, and abdomen).
Results: After the literature scrutinization (n = 1008), 52 papers were recognized for the systematic review. Nine studies of dosimtric studies and eleven studies of geometric analysis were suitable for inclusion in meta-analysis. Using kVCBCT for treatment replanning depends on a method used. Deformable Image Registration (DIR) methods yielded small dosimetric error (≤2%), γ pass rate (≥90%) and DSC (≥0.8). Hounsfield Unit (HU) override and calibration curve-based methods also achieved satisfactory yielded small dosimetric error (≤2%) and γ pass rate ((≥90%), but they are prone to error due to their sensitivity to a vendor-specific variation in kVCBCT image quality.
Conclusions: Large cohorts of patients ought to be undertaken to validate methods achieving low levels of dosimetric and geometric errors. Quality guidelines should be established when reporting on kVCBCT, which include agreed metrics for reporting on the quality of corrected kVCBCT and defines protocols of new site-specific standardized imaging used when obtaining kVCBCT images for adaptive radiotherapy.
Advances in knowledge: This review gives useful knowledge about methods making kVCBCT feasible for kVCBCT-based adaptive radiotherapy, simplifying patient pathway and reducing concomitant imaging dose to the patient.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


