Max Miller, Nancy H Kim, Maya K Thosani, Justin C Moser
{"title":"Use of Talimogene Laherparepvec to Treat Cutaneous Squamous Cell Carcinoma in a Renal Transplant Patient.","authors":"Max Miller, Nancy H Kim, Maya K Thosani, Justin C Moser","doi":"10.1159/000530851","DOIUrl":null,"url":null,"abstract":"<p><p>A 66-year-old female with a history of two renal transplants due to recurrent thrombotic thrombocytopenic purpura presented to clinic with multiple lesions identified to be non-metastatic cutaneous squamous cell carcinoma (CSCC). The patient previously underwent multiple Mohs procedures and radiation therapy treatment but continued to develop CSCC lesions with increasing frequency. After discussing multiple treatment options, it was elected to pursue treatment with Talimogene laherparepvec (T-VEC) given the systemic immune responses it can cause, with low theoretical risk of graft rejection. After starting intratumoral T-VEC injections, treated lesions began to decrease in size, and a reduction in the rate of new CSCC lesions was observed. Treatment was held due to unrelated renal complications during which time new CSCCs developed. Patient was restarted on T-VEC therapy with no recurrent renal issues. Upon reinitiating treatment, injected and non-injected lesions showed reduction in size, and the development of new lesions again ceased. One injected lesion was resected via Mohs micrographic surgery due to its size and discomfort. On sectioning, this demonstrated an exuberant lymphocytic perivascular infiltrate which was consistent with treatment response to T-VEC, with little active tumor. With high rates of non-melanoma skin cancer in renal transplant patients, their transplant status significantly limits treatment options, specifically with regards to anti-PD-1 therapy. This case suggests T-VEC can generate local and systemic immune responses in the setting of immunosuppression and that T-VEC may be a beneficial therapeutic option for transplant patients with CSCC.</p>","PeriodicalId":9619,"journal":{"name":"Case Reports in Dermatology","volume":"15 1","pages":"99-104"},"PeriodicalIF":0.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10294262/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Dermatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000530851","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
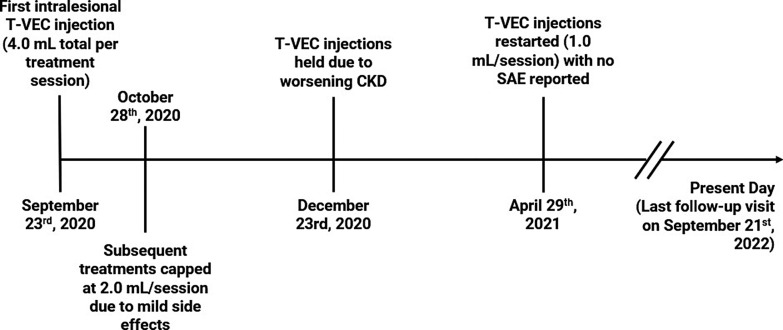
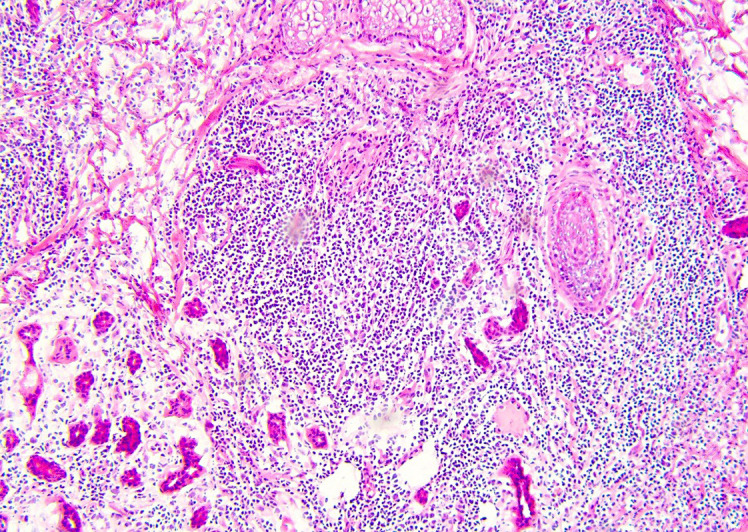
A 66-year-old female with a history of two renal transplants due to recurrent thrombotic thrombocytopenic purpura presented to clinic with multiple lesions identified to be non-metastatic cutaneous squamous cell carcinoma (CSCC). The patient previously underwent multiple Mohs procedures and radiation therapy treatment but continued to develop CSCC lesions with increasing frequency. After discussing multiple treatment options, it was elected to pursue treatment with Talimogene laherparepvec (T-VEC) given the systemic immune responses it can cause, with low theoretical risk of graft rejection. After starting intratumoral T-VEC injections, treated lesions began to decrease in size, and a reduction in the rate of new CSCC lesions was observed. Treatment was held due to unrelated renal complications during which time new CSCCs developed. Patient was restarted on T-VEC therapy with no recurrent renal issues. Upon reinitiating treatment, injected and non-injected lesions showed reduction in size, and the development of new lesions again ceased. One injected lesion was resected via Mohs micrographic surgery due to its size and discomfort. On sectioning, this demonstrated an exuberant lymphocytic perivascular infiltrate which was consistent with treatment response to T-VEC, with little active tumor. With high rates of non-melanoma skin cancer in renal transplant patients, their transplant status significantly limits treatment options, specifically with regards to anti-PD-1 therapy. This case suggests T-VEC can generate local and systemic immune responses in the setting of immunosuppression and that T-VEC may be a beneficial therapeutic option for transplant patients with CSCC.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


