Abdelwahap Elghezewi, Mohamad Hammad, Mohammed El-Dallal, Mujtaba Mohamed, Ahmed Sherif, Wesam Frandah
{"title":"Trends in Hospitalizations of Esophageal Varices From 2011 to 2018: A United States Nationwide Study.","authors":"Abdelwahap Elghezewi, Mohamad Hammad, Mohammed El-Dallal, Mujtaba Mohamed, Ahmed Sherif, Wesam Frandah","doi":"10.14740/gr1627","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prevalence of gastroesophageal varices is around 50% of patients with cirrhosis. In compensated cirrhosis they are present in 30-40%. Progression from small to large varices occurs at rate of 10-12% annually. That percentage increases significantly in decompensated liver cirrhosis with gastroesophageal varices found in 85% of patients. Variceal hemorrhage occurs at a rate around 10-15% per year. The outcome of variceal hemorrhage depends on the severity of liver disease, size of varices, and presence of stigmata of recent bleeding (red whale sign). Six-week mortality of variceal hemorrhage ranges between 15% and 25%. Without treatment, variceal hemorrhage tends to recur in 60% of patients within 1 - 2 years. The aim of the study was to assess demographics of esophageal varices with and without bleeding, geographic distribution, comorbidities, outcomes, main payers, and cost of hospitalizations.</p><p><strong>Methods: </strong>The National Inpatient Sample (NIS) database from year 2011 to 2018 was used. Patients who had a primary diagnosis of esophageal varices with or without bleeding were identified using the International Classification of Diseases, Ninth Revision (ICD-9) codes (456.0 for esophageal varices with bleeding, and 456.1 for esophageal varices without bleeding), and International Classification of Diseases, 10th Revision (ICD-10) codes (I85.01 for esophageal varices with bleeding, and I85.00 for esophageal varices without bleeding) in the first two discharge diagnoses. The propensity score to calculate the inverse probability treatment weighting (IPTW) to adjust between the differences of the compared groups was implemented. Two groups were compared in terms of their hospitalization outcomes, including LOS, hospital charges, hospital mortality, and disposition.</p><p><strong>Results: </strong>A total of 322,761 patients were admitted with esophageal varices between 2011 and 2018, with 236,802 (73.6%) had bleeding esophageal varices and 85,959 (26.4%) had nonbleeding esophageal varices. The majority of the patients from both groups were white (66%), covered with Medicare (38% in the esophageal varices with bleeding vs. 41% in the nonbleeding group). There was a steady increase of patients admitted with nonbleeding esophageal varices. Most common comorbidities were liver diseases, alcohol abuse, uncomplicated hypertension and depression in both groups. There were no significant changes in OLS over the years in both groups, but there was a significant increase in hospital charges, especially in the patients with bleeding esophageal varices starting in 2015, and no change in mortality throughout the years. Regarding hospital disposition, there was a notable decline in rehab discharge in the bleeding esophageal varices group.</p><p><strong>Conclusions: </strong>Esophageal varices with and without bleeding have been steadily increasing since the beginning of this century. This may result in a substantial impact on increasing health care costs and utilization due to acute variceal hemorrhage. Odds of death, transfer to urban hospital, and transfer to visiting nursing assistance remained unchanged.</p>","PeriodicalId":12461,"journal":{"name":"Gastroenterology Research","volume":"16 3","pages":"171-183"},"PeriodicalIF":1.7000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c6/56/gr-16-171.PMC10284649.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastroenterology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/gr1627","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Prevalence of gastroesophageal varices is around 50% of patients with cirrhosis. In compensated cirrhosis they are present in 30-40%. Progression from small to large varices occurs at rate of 10-12% annually. That percentage increases significantly in decompensated liver cirrhosis with gastroesophageal varices found in 85% of patients. Variceal hemorrhage occurs at a rate around 10-15% per year. The outcome of variceal hemorrhage depends on the severity of liver disease, size of varices, and presence of stigmata of recent bleeding (red whale sign). Six-week mortality of variceal hemorrhage ranges between 15% and 25%. Without treatment, variceal hemorrhage tends to recur in 60% of patients within 1 - 2 years. The aim of the study was to assess demographics of esophageal varices with and without bleeding, geographic distribution, comorbidities, outcomes, main payers, and cost of hospitalizations.
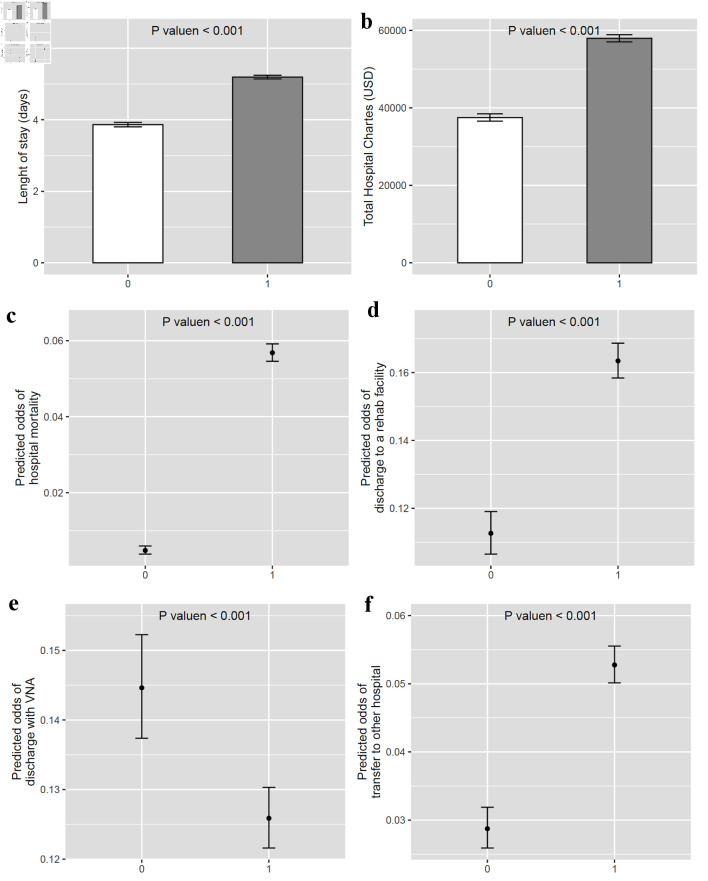
Methods: The National Inpatient Sample (NIS) database from year 2011 to 2018 was used. Patients who had a primary diagnosis of esophageal varices with or without bleeding were identified using the International Classification of Diseases, Ninth Revision (ICD-9) codes (456.0 for esophageal varices with bleeding, and 456.1 for esophageal varices without bleeding), and International Classification of Diseases, 10th Revision (ICD-10) codes (I85.01 for esophageal varices with bleeding, and I85.00 for esophageal varices without bleeding) in the first two discharge diagnoses. The propensity score to calculate the inverse probability treatment weighting (IPTW) to adjust between the differences of the compared groups was implemented. Two groups were compared in terms of their hospitalization outcomes, including LOS, hospital charges, hospital mortality, and disposition.
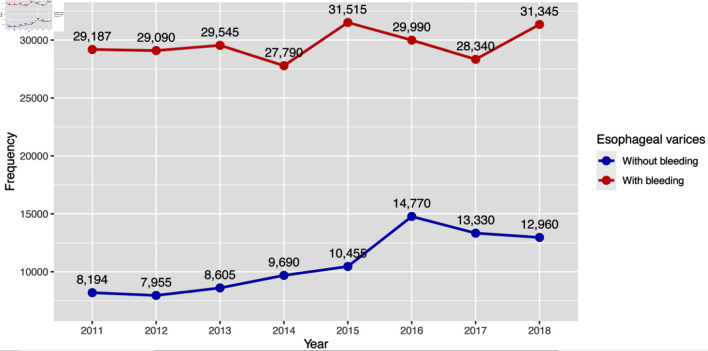
Results: A total of 322,761 patients were admitted with esophageal varices between 2011 and 2018, with 236,802 (73.6%) had bleeding esophageal varices and 85,959 (26.4%) had nonbleeding esophageal varices. The majority of the patients from both groups were white (66%), covered with Medicare (38% in the esophageal varices with bleeding vs. 41% in the nonbleeding group). There was a steady increase of patients admitted with nonbleeding esophageal varices. Most common comorbidities were liver diseases, alcohol abuse, uncomplicated hypertension and depression in both groups. There were no significant changes in OLS over the years in both groups, but there was a significant increase in hospital charges, especially in the patients with bleeding esophageal varices starting in 2015, and no change in mortality throughout the years. Regarding hospital disposition, there was a notable decline in rehab discharge in the bleeding esophageal varices group.
Conclusions: Esophageal varices with and without bleeding have been steadily increasing since the beginning of this century. This may result in a substantial impact on increasing health care costs and utilization due to acute variceal hemorrhage. Odds of death, transfer to urban hospital, and transfer to visiting nursing assistance remained unchanged.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


