Veena Iyer, Gulrez Shah Azhar, Nandini Choudhury, Vidwan Singh Dhruwey, Russell Dacombe, Ashish Upadhyay
{"title":"Infectious disease burden in Gujarat (2005-2011): comparison of selected infectious disease rates with India.","authors":"Veena Iyer, Gulrez Shah Azhar, Nandini Choudhury, Vidwan Singh Dhruwey, Russell Dacombe, Ashish Upadhyay","doi":"10.3402/ehtj.v7.22838","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>India is known to be endemic to numerous infectious diseases. The infectious disease profile of India is changing due to increased human environmental interactions, urbanisation and climate change. There are also predictions of explosive growth in infectious and zoonotic diseases. The Integrated Disease Surveillance Project (IDSP) was implemented in Gujarat in 2004.</p><p><strong>Methods: </strong>We analysed IDSP data on seven laboratory confirmed infectious diseases from 2005-2011 on temporal and spatial trends and compared this to the National Health Profile (NHP) data for the same period and with other literature. We chose laboratory cases data for Enteric fever, Cholera, Hepatitis, Dengue, Chikungunya, Measles and Diphtheria in the state since well designed vertical programs do not exist for these diseases. Statistical and GIS analysis was done using appropriate software.</p><p><strong>Results: </strong>Our analysis shows that the existing surveillance system in the state is predominantly reporting urban cases. There are wide variations among reported cases within the state with reports of Enteric fever and Measles being less than half of the national average, while Cholera, Viral Hepatitis and Dengue being nearly double.</p><p><strong>Conclusions: </strong>We found some limitations in the IDSP system with regard to the number of reporting units and cases in the background of a mixed health system with multiplicity of treatment providers and payment mechanisms. Despite these limitations, IDSP can be strengthened into a comprehensive surveillance system capable of tackling the challenge of reversing the endemicity of these diseases and preventing the emergence of others.</p>","PeriodicalId":72898,"journal":{"name":"Emerging health threats journal","volume":"7 ","pages":"22838"},"PeriodicalIF":0.0000,"publicationDate":"2014-03-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3962030/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Emerging health threats journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3402/ehtj.v7.22838","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: India is known to be endemic to numerous infectious diseases. The infectious disease profile of India is changing due to increased human environmental interactions, urbanisation and climate change. There are also predictions of explosive growth in infectious and zoonotic diseases. The Integrated Disease Surveillance Project (IDSP) was implemented in Gujarat in 2004.
Methods: We analysed IDSP data on seven laboratory confirmed infectious diseases from 2005-2011 on temporal and spatial trends and compared this to the National Health Profile (NHP) data for the same period and with other literature. We chose laboratory cases data for Enteric fever, Cholera, Hepatitis, Dengue, Chikungunya, Measles and Diphtheria in the state since well designed vertical programs do not exist for these diseases. Statistical and GIS analysis was done using appropriate software.
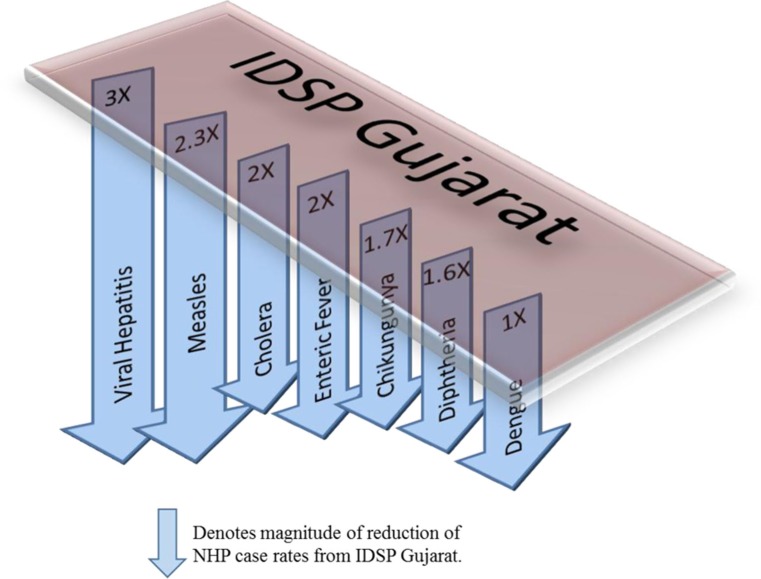
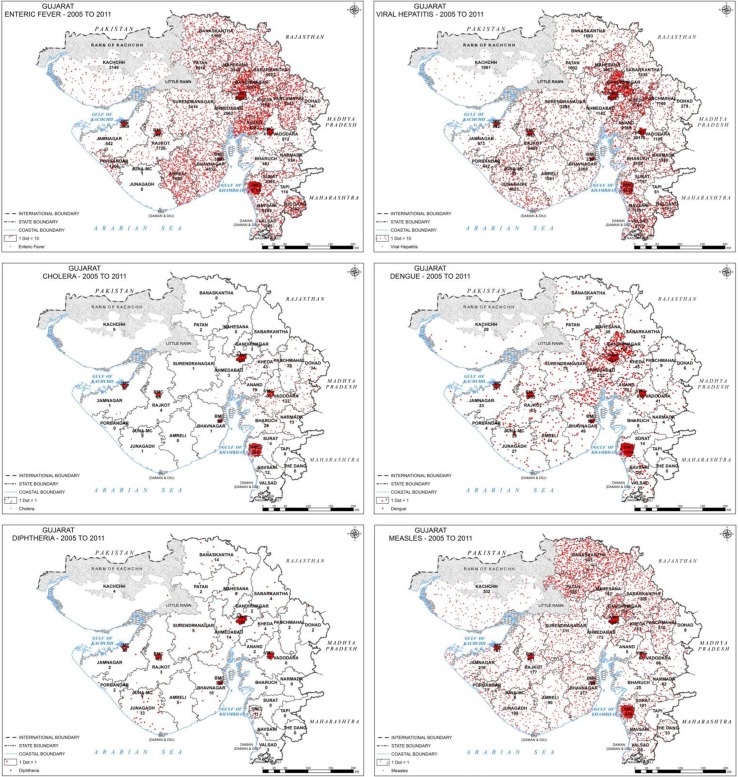
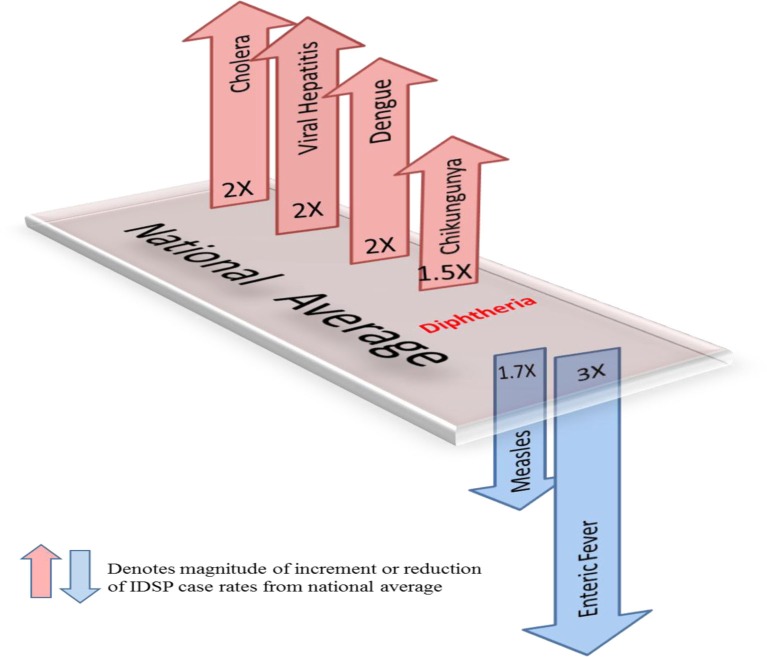
Results: Our analysis shows that the existing surveillance system in the state is predominantly reporting urban cases. There are wide variations among reported cases within the state with reports of Enteric fever and Measles being less than half of the national average, while Cholera, Viral Hepatitis and Dengue being nearly double.
Conclusions: We found some limitations in the IDSP system with regard to the number of reporting units and cases in the background of a mixed health system with multiplicity of treatment providers and payment mechanisms. Despite these limitations, IDSP can be strengthened into a comprehensive surveillance system capable of tackling the challenge of reversing the endemicity of these diseases and preventing the emergence of others.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


