Ismail Ghafary, Chang-Kyung Kim, Eric Roth, Michael Lu, Erin M Taub, Susan Lee, Ira Cohen, Zhongju Lu
{"title":"The association of QTc prolongation with cardiovascular events in cancer patients taking tyrosine kinase inhibitors (TKIs).","authors":"Ismail Ghafary, Chang-Kyung Kim, Eric Roth, Michael Lu, Erin M Taub, Susan Lee, Ira Cohen, Zhongju Lu","doi":"10.1186/s40959-023-00178-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To investigate the association between stages of QTc prolongation and the risk of cardiac events among patients on TKIs.</p><p><strong>Methods: </strong>This was a retrospective cohort study performed at an academic tertiary care center of cancer patients who were taking TKIs or not taking TKIs. Patients with two recorded ECGs between January 1, 2009, and December 31, 2019, were selected from an electronic database. The QTc duration > 450ms was determined as prolonged. The association between QTc prolongation progression and events of cardiovascular disease were compared.</p><p><strong>Results: </strong>This study included a total of 451 patients with 41.2% of patients taking TKIs. During a median follow up period of 3.1 years, 49.5% subjects developed CVD and 5.4% subjects suffered cardiac death in patient using TKIs (n = 186); the corresponding rates are 64.2% and 1.2% for patients not on TKIs (n = 265), respectively. Among patient on TKIs, 4.8% of subjects developed stroke, 20.4% of subjects suffered from heart failure (HF) and 24.2% of subjects had myocardial infarction (MI); corresponding incidence are 6.8%, 26.8% and 30.6% in non-TKIs. When patients were regrouped to TKIs versus non-TKIs with and without diabetes, there was no significant difference in the incidence of cardiac events among all groups. Adjusted Cox proportional hazards models were applied to estimate hazard ratios (HRs) with 95% confidence intervals (CIs). There is a significant increased risk of HF events (HR, 95% CI: 2.12, 1.36-3.32) and MI events (HR, 95% CI: 1.78, 1.16-2.73) during the 1st visit. There are also trends for an increased incidence of cardiac adverse events associated with QTc prolongation among patient with QTc > 450ms, however the difference is not statistically significant. Increased cardiac adverse events in patients with QTc prolongation were reproduced during the 2nd visit and the incidence of heart failure was significantly associated with QTc prolongation(HR, 95% CI: 2.94, 1.73-5.0).</p><p><strong>Conclusion: </strong>There is a significant increased QTc prolongation in patients taking TKIs. QTc prolongation caused by TKIs is associated with an increased risk of cardiac events.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":null,"pages":null},"PeriodicalIF":3.2000,"publicationDate":"2023-05-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10197472/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-023-00178-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To investigate the association between stages of QTc prolongation and the risk of cardiac events among patients on TKIs.
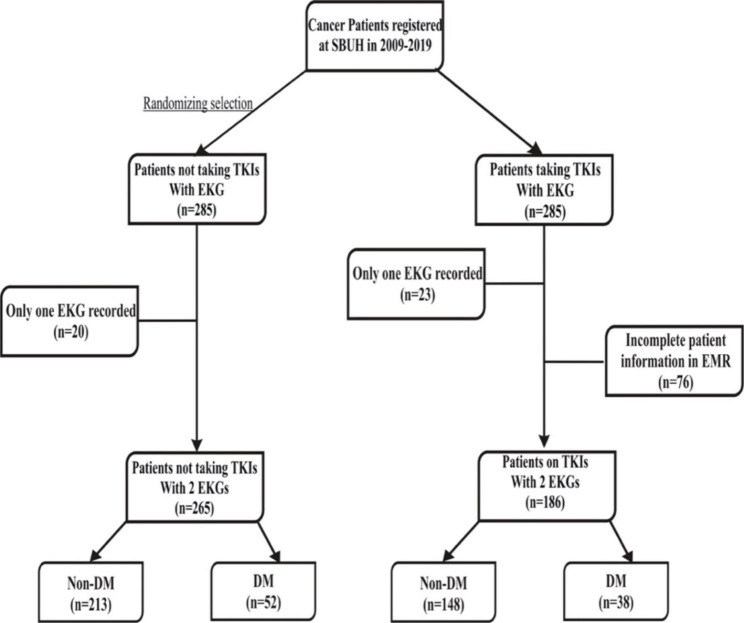
Methods: This was a retrospective cohort study performed at an academic tertiary care center of cancer patients who were taking TKIs or not taking TKIs. Patients with two recorded ECGs between January 1, 2009, and December 31, 2019, were selected from an electronic database. The QTc duration > 450ms was determined as prolonged. The association between QTc prolongation progression and events of cardiovascular disease were compared.
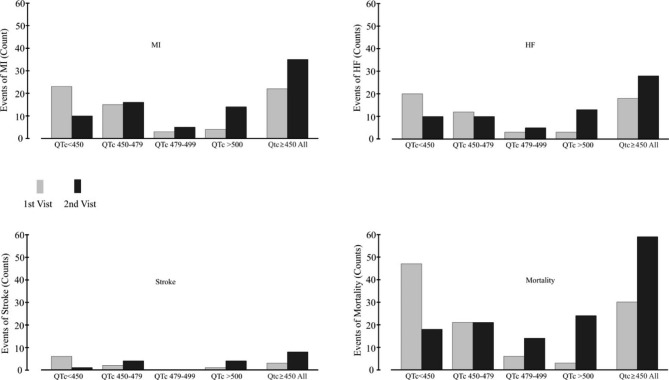
Results: This study included a total of 451 patients with 41.2% of patients taking TKIs. During a median follow up period of 3.1 years, 49.5% subjects developed CVD and 5.4% subjects suffered cardiac death in patient using TKIs (n = 186); the corresponding rates are 64.2% and 1.2% for patients not on TKIs (n = 265), respectively. Among patient on TKIs, 4.8% of subjects developed stroke, 20.4% of subjects suffered from heart failure (HF) and 24.2% of subjects had myocardial infarction (MI); corresponding incidence are 6.8%, 26.8% and 30.6% in non-TKIs. When patients were regrouped to TKIs versus non-TKIs with and without diabetes, there was no significant difference in the incidence of cardiac events among all groups. Adjusted Cox proportional hazards models were applied to estimate hazard ratios (HRs) with 95% confidence intervals (CIs). There is a significant increased risk of HF events (HR, 95% CI: 2.12, 1.36-3.32) and MI events (HR, 95% CI: 1.78, 1.16-2.73) during the 1st visit. There are also trends for an increased incidence of cardiac adverse events associated with QTc prolongation among patient with QTc > 450ms, however the difference is not statistically significant. Increased cardiac adverse events in patients with QTc prolongation were reproduced during the 2nd visit and the incidence of heart failure was significantly associated with QTc prolongation(HR, 95% CI: 2.94, 1.73-5.0).
Conclusion: There is a significant increased QTc prolongation in patients taking TKIs. QTc prolongation caused by TKIs is associated with an increased risk of cardiac events.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


