Georgios P Skandalakis, Aristotelis Kalyvas, Evgenia Lani, Spyridon Komaitis, Danai Manolakou, Despoina Chatzopoulou, Nikos Pantazis, Georgios A Zenonos, Constantinos G Hadjipanayis, George Stranjalis, Christos Koutsarnakis
{"title":"Effectiveness of pharmacologic interventions for prevention of cerebral hyperperfusion syndrome following bypass surgery.","authors":"Georgios P Skandalakis, Aristotelis Kalyvas, Evgenia Lani, Spyridon Komaitis, Danai Manolakou, Despoina Chatzopoulou, Nikos Pantazis, Georgios A Zenonos, Constantinos G Hadjipanayis, George Stranjalis, Christos Koutsarnakis","doi":"10.4103/bc.bc_43_22","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cerebral hyperperfusion syndrome (CHS) following bypass surgery is a major cause of neurological morbidity and mortality. However, data regarding its prevention have not been assorted until date.</p><p><strong>Objective: </strong>The objective of this study was to review the literature and evaluate whether any conclusion can be drawn regarding the effectiveness of any measure on preventing bypass-related CHS.</p><p><strong>Methods: </strong>We systematically reviewed PubMed and Cochrane Library from September 2008 to September 2018 to collect data regarding the effectiveness of pharmacologic interventions on the refers to pretreatment (PRE) of bypass-related CHS. We categorized interventions regarding their class of drugs and their combinations and calculated overall pooled estimates of proportions of CHS development through random-effects meta-analysis of proportions.</p><p><strong>Results: </strong>Our search yielded 649 studies, of which 23 fulfilled inclusion criteria. Meta-analysis included 23 studies/2,041 cases. In Group A (blood pressure [BP] control), 202 out of 1,174 pretreated cases developed CHS (23.3% pooled estimate; 95% confidence interval [CI]: 9.9-39.4), Group B (BP control + free radical scavenger [FRS]) 10/263 (0.3%; 95% CI: 0.0-14.1), Group C (BP control + antiplatelet) 22/204 (10.3%; 95% CI: 5.1-16.7), and Group D (BP control + postoperative sedation) 29/400 (6.8%; 95% CI: 4.4-9.6)].</p><p><strong>Conclusions: </strong>BP control alone has not been proven effective in preventing CHS. However, BP control along with either a FRS or an antiplatelet agent or postoperative sedation seems to reduce the incidence of CHS.</p>","PeriodicalId":9288,"journal":{"name":"Brain Circulation","volume":"8 4","pages":"207-214"},"PeriodicalIF":4.8000,"publicationDate":"2022-12-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5c/e8/BC-8-207.PMC10167845.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain Circulation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4103/bc.bc_43_22","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cerebral hyperperfusion syndrome (CHS) following bypass surgery is a major cause of neurological morbidity and mortality. However, data regarding its prevention have not been assorted until date.
Objective: The objective of this study was to review the literature and evaluate whether any conclusion can be drawn regarding the effectiveness of any measure on preventing bypass-related CHS.
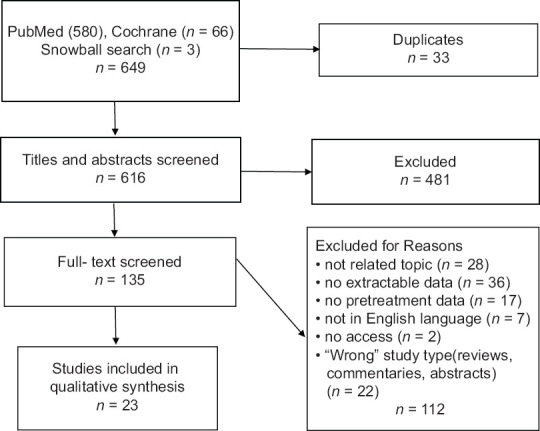
Methods: We systematically reviewed PubMed and Cochrane Library from September 2008 to September 2018 to collect data regarding the effectiveness of pharmacologic interventions on the refers to pretreatment (PRE) of bypass-related CHS. We categorized interventions regarding their class of drugs and their combinations and calculated overall pooled estimates of proportions of CHS development through random-effects meta-analysis of proportions.
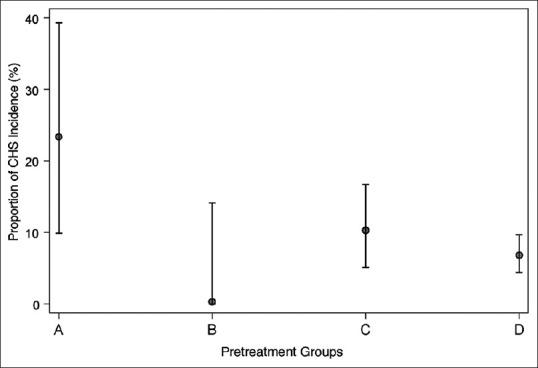
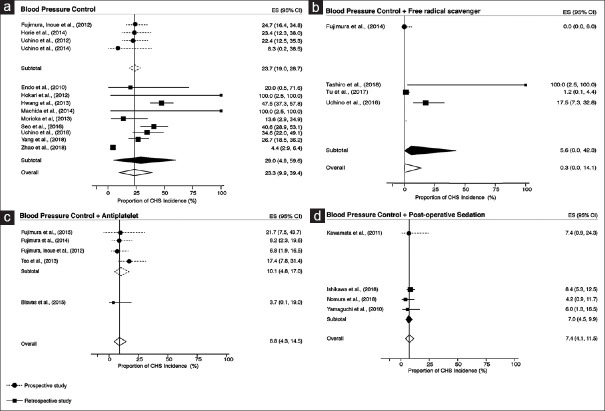
Results: Our search yielded 649 studies, of which 23 fulfilled inclusion criteria. Meta-analysis included 23 studies/2,041 cases. In Group A (blood pressure [BP] control), 202 out of 1,174 pretreated cases developed CHS (23.3% pooled estimate; 95% confidence interval [CI]: 9.9-39.4), Group B (BP control + free radical scavenger [FRS]) 10/263 (0.3%; 95% CI: 0.0-14.1), Group C (BP control + antiplatelet) 22/204 (10.3%; 95% CI: 5.1-16.7), and Group D (BP control + postoperative sedation) 29/400 (6.8%; 95% CI: 4.4-9.6)].
Conclusions: BP control alone has not been proven effective in preventing CHS. However, BP control along with either a FRS or an antiplatelet agent or postoperative sedation seems to reduce the incidence of CHS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


