{"title":"Diagnostic and Management Strategies of IgA Vasculitis Nephritis/Henoch-Schönlein Purpura Nephritis in Pediatric Patients: Current Perspectives.","authors":"Mario Sestan, Marija Jelusic","doi":"10.2147/PHMT.S379862","DOIUrl":null,"url":null,"abstract":"<p><p>IgA vasculitis (IgAV) or Henoch-Schönlein purpura (HSP) is the most common vasculitis in children, and nephritis (IgAVN or HSPN) is the most important and only chronic manifestation of the disease. Despite this, there are no diagnostic criteria and we rely on the European League Against Rheumatism/Paediatric Rheumatology International Trials Organization/Paediatric Rheumatology European Society-endorsed Ankara 2008 classification criteria in our daily practice. Basic investigations that should be done in every patient with IgAVN include blood pressure measurement, estimated glomerular filtration rate and urinalysis. Kidney biopsy is still the gold standard for the diagnosis of IgAVN since noninvasive confirmation of nephritis is still pending. According to the Single Hub and Access point for pediatric Rheumatology in Europe (SHARE) recommendations, the first-line treatment for with mild forms of IgAVN is oral glucocorticoids, for patients with moderate IgAVN parenterally administrated glucocorticoids in pulsed doses, while initial treatment for patients with the most severe forms of IgAVN include pulsed doses of glucocorticoids in combination with intravenous cyclophosphamide pulses. New therapeutic options are currently being tested, aiming to reduce the production of galactose-deficient IgA<sub>1</sub> and autoantibodies or suppress the alternative or lectin complement pathway and blocking mesangial cell activation.</p>","PeriodicalId":74410,"journal":{"name":"Pediatric health, medicine and therapeutics","volume":"14 ","pages":"89-98"},"PeriodicalIF":1.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ed/49/phmt-14-89.PMC10008002.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric health, medicine and therapeutics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/PHMT.S379862","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
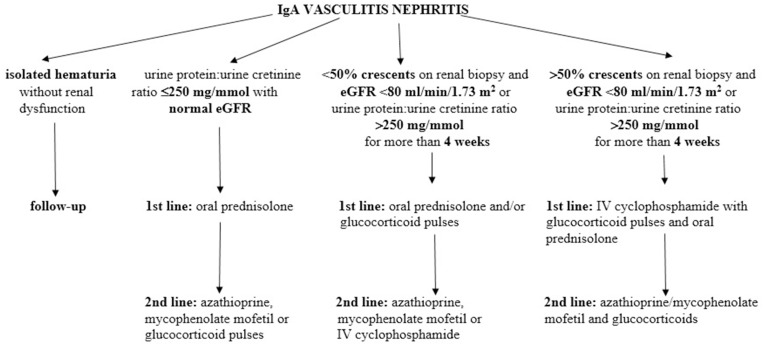
IgA vasculitis (IgAV) or Henoch-Schönlein purpura (HSP) is the most common vasculitis in children, and nephritis (IgAVN or HSPN) is the most important and only chronic manifestation of the disease. Despite this, there are no diagnostic criteria and we rely on the European League Against Rheumatism/Paediatric Rheumatology International Trials Organization/Paediatric Rheumatology European Society-endorsed Ankara 2008 classification criteria in our daily practice. Basic investigations that should be done in every patient with IgAVN include blood pressure measurement, estimated glomerular filtration rate and urinalysis. Kidney biopsy is still the gold standard for the diagnosis of IgAVN since noninvasive confirmation of nephritis is still pending. According to the Single Hub and Access point for pediatric Rheumatology in Europe (SHARE) recommendations, the first-line treatment for with mild forms of IgAVN is oral glucocorticoids, for patients with moderate IgAVN parenterally administrated glucocorticoids in pulsed doses, while initial treatment for patients with the most severe forms of IgAVN include pulsed doses of glucocorticoids in combination with intravenous cyclophosphamide pulses. New therapeutic options are currently being tested, aiming to reduce the production of galactose-deficient IgA1 and autoantibodies or suppress the alternative or lectin complement pathway and blocking mesangial cell activation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


