Elizabeth O'Connor, Ryo Tamura, Therese Hannon, Sundeep Harigopal, Bruce Jaffray
{"title":"Congenital diaphragmatic hernia survival in an English regional ECMO center.","authors":"Elizabeth O'Connor, Ryo Tamura, Therese Hannon, Sundeep Harigopal, Bruce Jaffray","doi":"10.1136/wjps-2022-000506","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Congenital diaphragmatic hernia (CDH) remains a cause of neonatal death. Our aims are to describe contemporary rates of survival and the variables associated with this outcome, contrasting these with our study of two decades earlier and recent reports.</p><p><strong>Materials and methods: </strong>A retrospective review of all infants diagnosed in a regional center between January 2000 and December 2020 was performed. The outcome of interest was survival. Possible explanatory variables included side of defect, use of complex ventilatory or hemodynamic strategies (inhaled nitric oxide (iNO), high-frequency oscillatory ventilation (HFOV), extracorporeal membrane oxygenation (ECMO), and Prostin), presence of antenatal diagnosis, associated anomalies, birth weight, and gestation. Temporal changes were studied by measuring outcomes in each of four consecutive 63-month periods.</p><p><strong>Results: </strong>A total of 225 cases were diagnosed. Survival was 60% (134 of 225). Postnatal survival was 68% (134 of 198 liveborn), and postrepair survival was 84% (134 of 159 who survived to repair). Diagnosis was made antenatally in 66% of cases. Variables associated with mortality were the need for complex ventilatory strategies (iNO, HFOV, Prostin, and ECMO), antenatal diagnosis, right-sided defects, use of patch repair, associated anomalies, birth weight, and gestation. Survival has improved from our report of a prior decade and did not vary during the study period. Postnatal survival has improved despite fewer terminations. On multivariate analysis, the need for complex ventilation was the strongest predictor of death (OR=50, 95% CI 13 to 224, p<0.0001), and associated anomalies ceased to be predictive.</p><p><strong>Conclusions: </strong>Survival has improved from our earlier report, despite reduced numbers of terminations. This may be related to increased use of complex ventilatory strategies.</p>","PeriodicalId":23823,"journal":{"name":"World Journal of Pediatric Surgery","volume":"6 2","pages":"e000506"},"PeriodicalIF":1.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ed/1b/wjps-2022-000506.PMC10152044.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Pediatric Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/wjps-2022-000506","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Congenital diaphragmatic hernia (CDH) remains a cause of neonatal death. Our aims are to describe contemporary rates of survival and the variables associated with this outcome, contrasting these with our study of two decades earlier and recent reports.
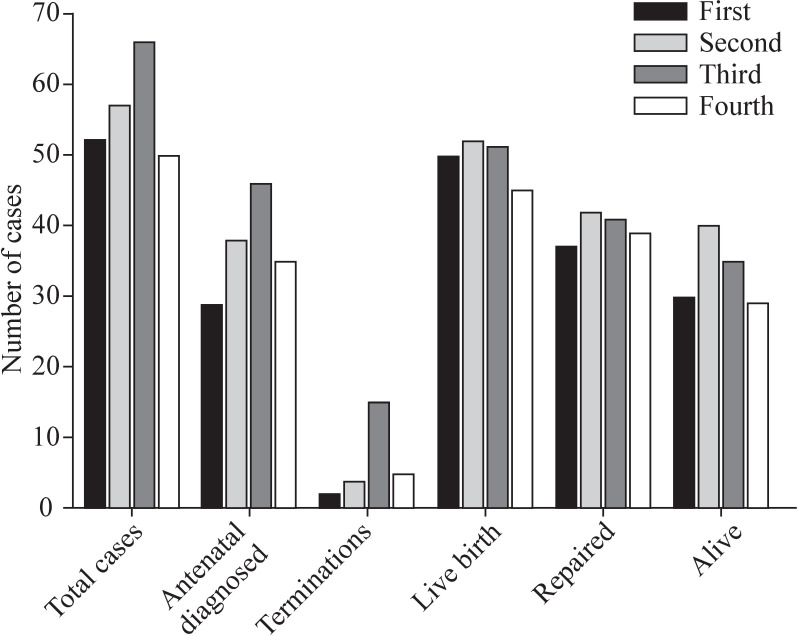
Materials and methods: A retrospective review of all infants diagnosed in a regional center between January 2000 and December 2020 was performed. The outcome of interest was survival. Possible explanatory variables included side of defect, use of complex ventilatory or hemodynamic strategies (inhaled nitric oxide (iNO), high-frequency oscillatory ventilation (HFOV), extracorporeal membrane oxygenation (ECMO), and Prostin), presence of antenatal diagnosis, associated anomalies, birth weight, and gestation. Temporal changes were studied by measuring outcomes in each of four consecutive 63-month periods.
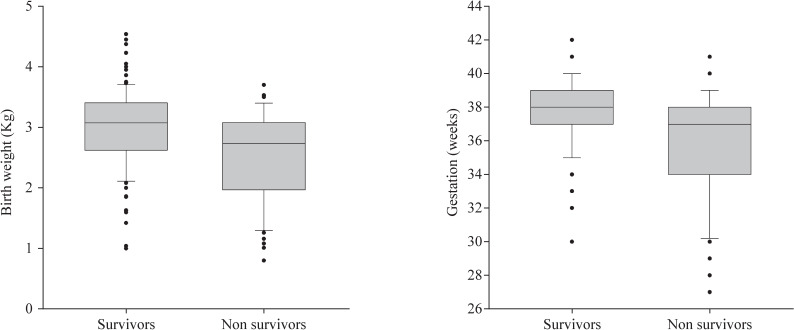
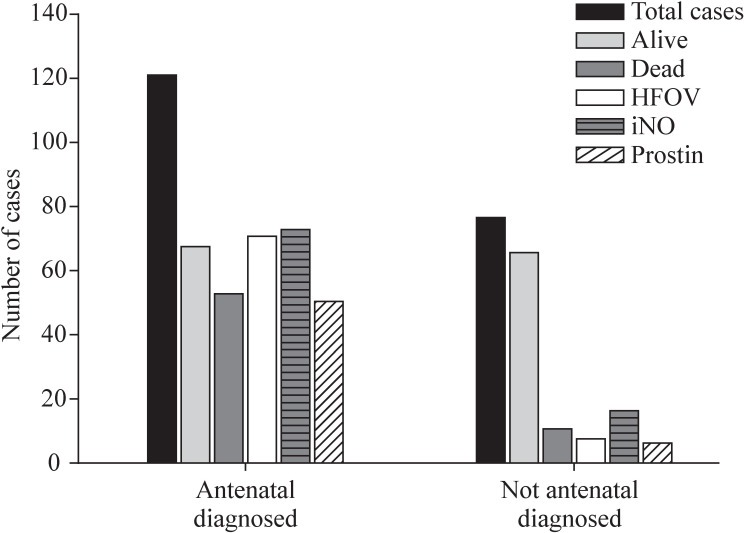
Results: A total of 225 cases were diagnosed. Survival was 60% (134 of 225). Postnatal survival was 68% (134 of 198 liveborn), and postrepair survival was 84% (134 of 159 who survived to repair). Diagnosis was made antenatally in 66% of cases. Variables associated with mortality were the need for complex ventilatory strategies (iNO, HFOV, Prostin, and ECMO), antenatal diagnosis, right-sided defects, use of patch repair, associated anomalies, birth weight, and gestation. Survival has improved from our report of a prior decade and did not vary during the study period. Postnatal survival has improved despite fewer terminations. On multivariate analysis, the need for complex ventilation was the strongest predictor of death (OR=50, 95% CI 13 to 224, p<0.0001), and associated anomalies ceased to be predictive.
Conclusions: Survival has improved from our earlier report, despite reduced numbers of terminations. This may be related to increased use of complex ventilatory strategies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


