{"title":"Percutaneous Trans-Esophageal Gastrostomy for Oral Intake in a Case of Anastomotic Obstruction following Total Gastrectomy.","authors":"Masayuki Shishida, Daisuke Sumitani, Masatsugu Yano, Makoto Ochi, Yuzo Okamoto, Shigeto Yoshida, Kazuaki Tanabe, Hideki Ohdan","doi":"10.1159/000530137","DOIUrl":null,"url":null,"abstract":"<p><p>Gastric cancer is one of the most common diseases globally. Total gastrectomy is often performed surgically. However, late-stage anastomotic passage obstruction after total gastrectomy is relatively rare. Here, we report a case involving a 73-year-old male patient who experienced repeated aspiration pneumonia due to anastomotic passage obstruction 22 years after a total gastrectomy for gastric cancer. He was eventually hospitalized in the Department of Gastroenterology at our hospital because of difficulty eating. Computed tomography revealed prominent dilation of the esophagus and the blind end of the elevated jejunum. Upper gastrointestinal endoscopy revealed a poorly extended site on the main side of the elevated jejunum; however, the passage through the scope was good. A percutaneous trans-esophageal gastrostomy was performed for oral intake. The patient experienced decreased nausea and vomiting. He gained weight, and his general condition improved. He did not feel inconvenienced by percutaneous trans-esophageal gastrostomy and had no desire for surgery. Follow-up observations are currently being conducted, with tubes exchanged every 6 months. There are no reports of percutaneous trans-esophageal gastrostomy for oral intake for anastomotic passage obstruction following total gastrectomy; therefore, we report this as a reference when similar cases are encountered.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"17 1","pages":"197-203"},"PeriodicalIF":0.5000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10116391/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000530137","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
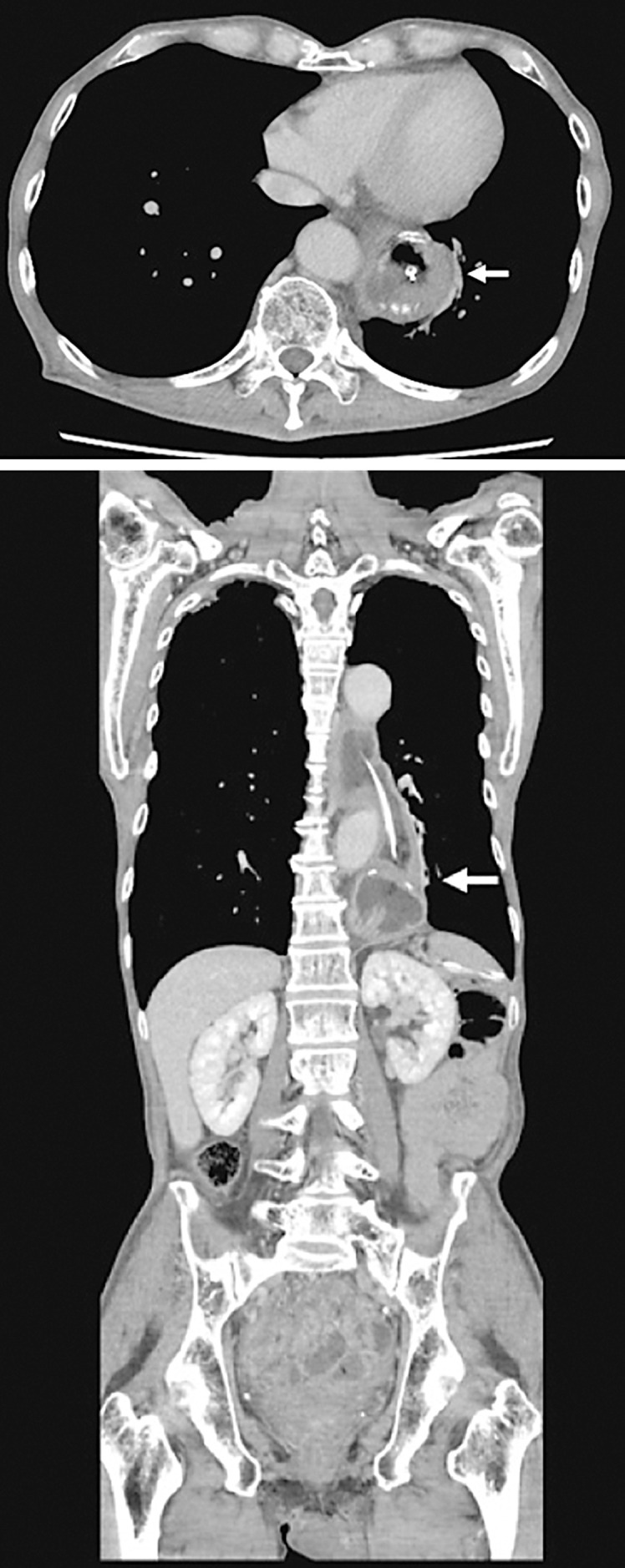
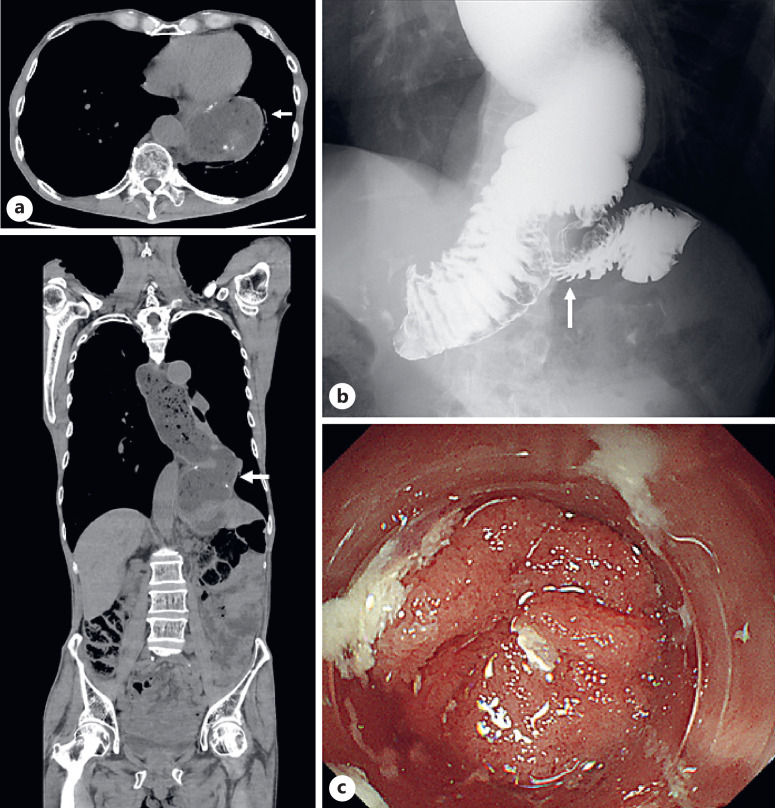
Gastric cancer is one of the most common diseases globally. Total gastrectomy is often performed surgically. However, late-stage anastomotic passage obstruction after total gastrectomy is relatively rare. Here, we report a case involving a 73-year-old male patient who experienced repeated aspiration pneumonia due to anastomotic passage obstruction 22 years after a total gastrectomy for gastric cancer. He was eventually hospitalized in the Department of Gastroenterology at our hospital because of difficulty eating. Computed tomography revealed prominent dilation of the esophagus and the blind end of the elevated jejunum. Upper gastrointestinal endoscopy revealed a poorly extended site on the main side of the elevated jejunum; however, the passage through the scope was good. A percutaneous trans-esophageal gastrostomy was performed for oral intake. The patient experienced decreased nausea and vomiting. He gained weight, and his general condition improved. He did not feel inconvenienced by percutaneous trans-esophageal gastrostomy and had no desire for surgery. Follow-up observations are currently being conducted, with tubes exchanged every 6 months. There are no reports of percutaneous trans-esophageal gastrostomy for oral intake for anastomotic passage obstruction following total gastrectomy; therefore, we report this as a reference when similar cases are encountered.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


