{"title":"Atrioventricular (AV) block and sinus arrest associated with dipyridamole infusion.","authors":"Mahdi Khalili, Mehrdad Jahani","doi":"10.48305/arya.v18i0.2381","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The use of dipyridamole for thallium-201 imaging has proved very successful in demonstrating coronary arterial disease, and a combination of dipyridamole and dynamic exercise is becoming widely used. Dipyridamole is safe when given intravenously, although transient noncardiac side effects are common; side effects such as chest pain, headache, and dizziness. These side effects are mostly mild, and can be treated with aminophylline.</p><p><strong>Case report: </strong>We describe a 45-year-old woman with normal baseline electrocardiography (ECG) and unremarkable physical examination, referred for myocardial thallium scan with dipyridamole. A few seconds after infusion of dipyridamole, her ECG developed first-degree atrioventricular (AV) block, then, 2:1 AV block, complete heart block (CHB), and sinus arrest. After aminophylline infusion, junctional escape rhythm was seen, and a few seconds later, rhythm changed to sinus rhythm. Thallium scan was negative for ischemia.</p><p><strong>Conclusion: </strong>High-grade AV block after dipyridamole has been described in few case reports, and mostly was associated with transient myocardial ischemia; it seems that the presence of conduction abnormalities at baseline is a risk factor. But in our case, the sinus arrest and AV block occurred without evidence of ischemia in myocardial perfusion imaging, and we think it can be an unwanted complication of dipyridamole; clinicians should be aware of bradyarrhythmia as a possible complication of dipyridamole. An alternative explanation is that this arrhythmia can be caused by vagal activity; and another possibility is that the imaging study was false negative.</p>","PeriodicalId":46477,"journal":{"name":"ARYA Atherosclerosis","volume":"18 3","pages":"1-3"},"PeriodicalIF":0.5000,"publicationDate":"2022-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a1/62/ARYA-18-9-2381.PMC9931949.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ARYA Atherosclerosis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.48305/arya.v18i0.2381","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The use of dipyridamole for thallium-201 imaging has proved very successful in demonstrating coronary arterial disease, and a combination of dipyridamole and dynamic exercise is becoming widely used. Dipyridamole is safe when given intravenously, although transient noncardiac side effects are common; side effects such as chest pain, headache, and dizziness. These side effects are mostly mild, and can be treated with aminophylline.
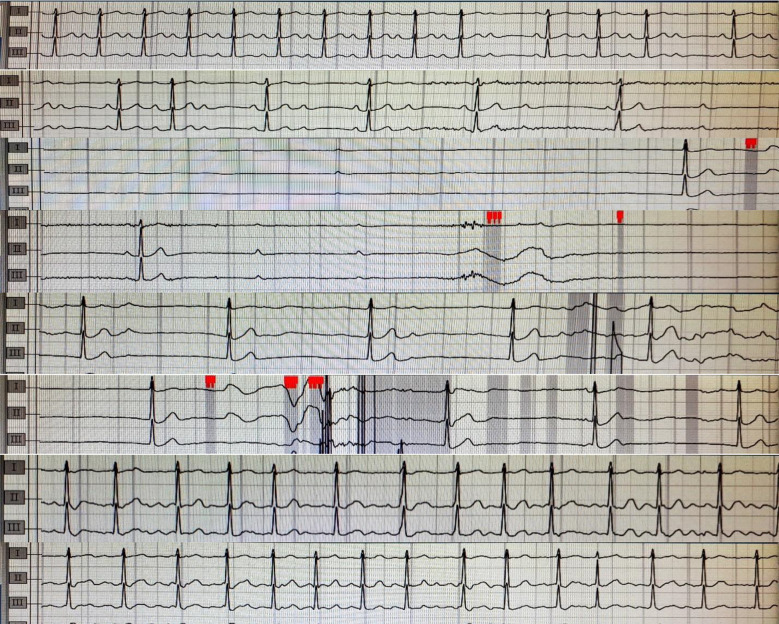
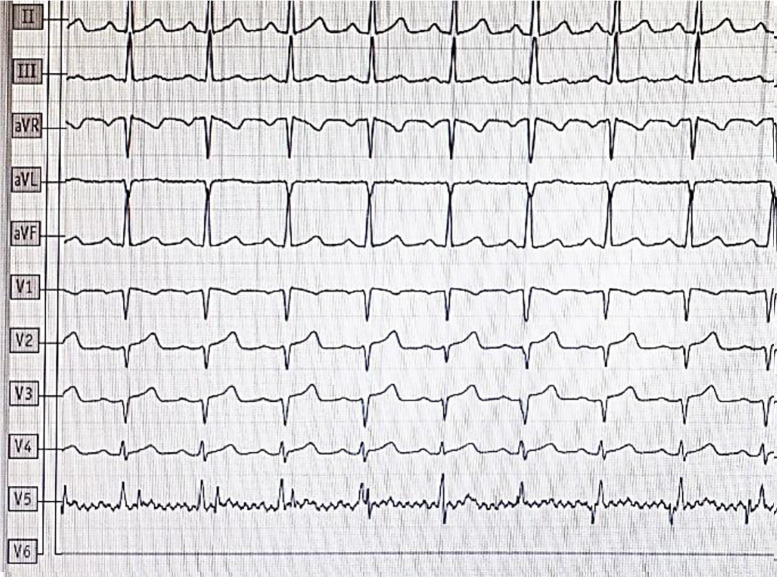
Case report: We describe a 45-year-old woman with normal baseline electrocardiography (ECG) and unremarkable physical examination, referred for myocardial thallium scan with dipyridamole. A few seconds after infusion of dipyridamole, her ECG developed first-degree atrioventricular (AV) block, then, 2:1 AV block, complete heart block (CHB), and sinus arrest. After aminophylline infusion, junctional escape rhythm was seen, and a few seconds later, rhythm changed to sinus rhythm. Thallium scan was negative for ischemia.
Conclusion: High-grade AV block after dipyridamole has been described in few case reports, and mostly was associated with transient myocardial ischemia; it seems that the presence of conduction abnormalities at baseline is a risk factor. But in our case, the sinus arrest and AV block occurred without evidence of ischemia in myocardial perfusion imaging, and we think it can be an unwanted complication of dipyridamole; clinicians should be aware of bradyarrhythmia as a possible complication of dipyridamole. An alternative explanation is that this arrhythmia can be caused by vagal activity; and another possibility is that the imaging study was false negative.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


