{"title":"Oral or Parenteral Methotrexate for the Treatment of Polyarticular Juvenile Idiopathic Arthritis.","authors":"Reima Bakry, Med A Klein, Gerd Horneff","doi":"10.5152/eurjrheum.2022.21090","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Subcutaneous methotrexate injections are considered to be more effective or work faster than oral methotrexate. Therefore, the extent and the kinetics of response were analyzed in juvenile idiopathic arthritis patients treated with oral versus subcutaneous methotrexate.</p><p><strong>Methods: </strong>The BIKER databank was searched for biologics-naive juvenile idiopathic arthritis patients treated with methotrexate as initial treatment. The Juvenile Arthritis Disease Activity Score-10 defini- tion of remission and the pediatric American College of Rheumatology's response parameters were utilized as outcome criteria.</p><p><strong>Result: </strong>A total of 410 polyarticular juvenile idiopathic arthritis patients receiving oral methotrexate were compared to 384 patients receiving subcutaneous methotrexate. Rheumatoid factor-negative polyarthritis was the most common juvenile idiopathic arthritis category (50%/51%) in this cohort followed by extended oligoarthritis (27%/26%), polyarticular psoriatic arthritis (18%/16%), and few had rheumatoid factor-positive polyarthritis (5%/8%). The oral cohort's disease duration (2.3 ± 3.0 vs. 1.9 ± 2.7) was significantly longer (P=.04), although their age at onset and baseline were similar. Furthermore, at baseline, disease activity (Juvenile Arthritis Disease Activity Score-10 16.5 ± 7.2 vs. 14.7 ± 8.2; P = .001 due to a higher active joint count 9.0 ± 10.1 vs. 7.4 ± 7.7; P = .011) was higher in the subcutaneous cohort. The weekly methotrexate doses were comparable with 13.6 ± 5.4 mg/m2 and 13.3 ± 4.5 mg/m2, respectively. With oral/subcutaneous methotrexate, a pediatric American College of Rheumatology's 90 was achieved in 98(38.3%)/128(40.4%), while 96(38.1 %)/75(40.1%) attained Juvenile Arthritis Disease Activity Score remission after 12 months of therapy. There was no difference in the early kinetics of response according to Kaplan-Meyer analysis. Adverse events including nausea, vomiting, and increased transaminases were considerably more common after methotrexate subcutaneous administration than after oral treatment.</p><p><strong>Conclusion: </strong>In terms of effectiveness, but not safety, our retrospective analysis found some advan- tages of subcutaneous methotrexate. Adverse effects limit treatment continuance and thus must be considered a disadvantage. Furthermore, oral methotrexate eliminates the need for injections, which is especially essential for younger children. Controlled, randomized prospective trials in children and juvenile patients are necessary for definitive recommendations for the subcutaneous route of admin- istration of methotrexate therapy.</p>","PeriodicalId":12066,"journal":{"name":"European journal of rheumatology","volume":"9 4","pages":"197-205"},"PeriodicalIF":1.8000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bf/05/ejr-9-4-197.PMC10089132.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5152/eurjrheum.2022.21090","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Subcutaneous methotrexate injections are considered to be more effective or work faster than oral methotrexate. Therefore, the extent and the kinetics of response were analyzed in juvenile idiopathic arthritis patients treated with oral versus subcutaneous methotrexate.
Methods: The BIKER databank was searched for biologics-naive juvenile idiopathic arthritis patients treated with methotrexate as initial treatment. The Juvenile Arthritis Disease Activity Score-10 defini- tion of remission and the pediatric American College of Rheumatology's response parameters were utilized as outcome criteria.
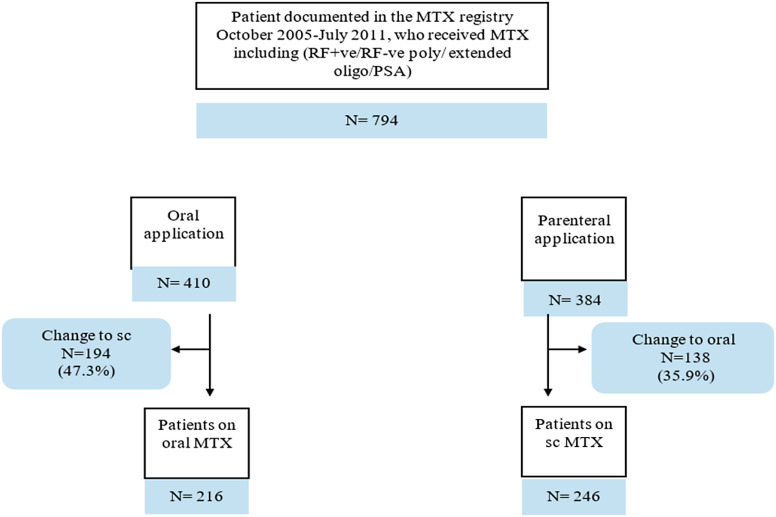
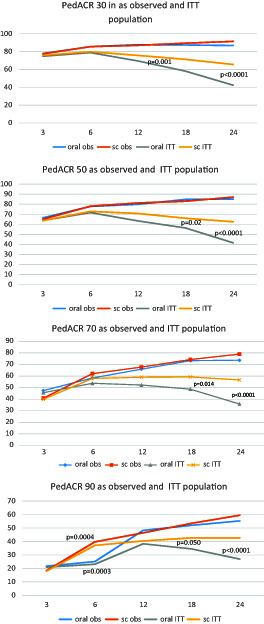
Result: A total of 410 polyarticular juvenile idiopathic arthritis patients receiving oral methotrexate were compared to 384 patients receiving subcutaneous methotrexate. Rheumatoid factor-negative polyarthritis was the most common juvenile idiopathic arthritis category (50%/51%) in this cohort followed by extended oligoarthritis (27%/26%), polyarticular psoriatic arthritis (18%/16%), and few had rheumatoid factor-positive polyarthritis (5%/8%). The oral cohort's disease duration (2.3 ± 3.0 vs. 1.9 ± 2.7) was significantly longer (P=.04), although their age at onset and baseline were similar. Furthermore, at baseline, disease activity (Juvenile Arthritis Disease Activity Score-10 16.5 ± 7.2 vs. 14.7 ± 8.2; P = .001 due to a higher active joint count 9.0 ± 10.1 vs. 7.4 ± 7.7; P = .011) was higher in the subcutaneous cohort. The weekly methotrexate doses were comparable with 13.6 ± 5.4 mg/m2 and 13.3 ± 4.5 mg/m2, respectively. With oral/subcutaneous methotrexate, a pediatric American College of Rheumatology's 90 was achieved in 98(38.3%)/128(40.4%), while 96(38.1 %)/75(40.1%) attained Juvenile Arthritis Disease Activity Score remission after 12 months of therapy. There was no difference in the early kinetics of response according to Kaplan-Meyer analysis. Adverse events including nausea, vomiting, and increased transaminases were considerably more common after methotrexate subcutaneous administration than after oral treatment.
Conclusion: In terms of effectiveness, but not safety, our retrospective analysis found some advan- tages of subcutaneous methotrexate. Adverse effects limit treatment continuance and thus must be considered a disadvantage. Furthermore, oral methotrexate eliminates the need for injections, which is especially essential for younger children. Controlled, randomized prospective trials in children and juvenile patients are necessary for definitive recommendations for the subcutaneous route of admin- istration of methotrexate therapy.
目的:甲氨蝶呤皮下注射被认为比口服甲氨蝶呤更有效或见效更快。因此,对口服甲氨蝶呤与皮下甲氨蝶呤治疗的青少年特发性关节炎患者的反应程度和动力学进行了分析。方法:检索BIKER数据库中以甲氨蝶呤为初始治疗的幼年特发性关节炎患者的生物制剂。儿童关节炎疾病活动度评分-10缓解定义和儿科美国风湿病学会的反应参数被用作结果标准。结果:410例接受口服甲氨蝶呤治疗的多关节幼年特发性关节炎患者与384例接受皮下甲氨蝶呤治疗的患者进行了比较。在该队列中,类风湿因子阴性的多发性关节炎是最常见的青少年特发性关节炎类型(50%/51%),其次是扩展性寡关节炎(27%/26%),多关节银屑病关节炎(18%/16%),少数类风湿因子阳性的多发性关节炎(5%/8%)。口腔组的疾病持续时间(2.3±3.0 vs 1.9±2.7)明显更长(P= 0.04),尽管他们的发病年龄和基线年龄相似。此外,在基线时,疾病活动性(青少年关节炎疾病活动性评分-10为16.5±7.2比14.7±8.2;P = 0.001,因为活动关节计数(9.0±10.1 vs. 7.4±7.7)较高;P = 0.011)在皮下组中更高。每周甲氨蝶呤剂量分别为13.6±5.4 mg/m2和13.3±4.5 mg/m2。口服/皮下甲氨蝶呤治疗12个月后,美国风湿病学会(American College of Rheumatology)的90名儿童中,98名(38.3%)/128名(40.4%)获得缓解,96名(38.1%)/75名(40.1%)获得青少年关节炎疾病活动评分缓解。根据Kaplan-Meyer分析,早期反应动力学没有差异。甲氨蝶呤皮下给药后,恶心、呕吐和转氨酶升高等不良事件比口服给药后更为常见。结论:从有效性而非安全性来看,我们的回顾性分析发现皮下甲氨蝶呤有一些优势。不良反应限制了治疗的持续,因此必须将其视为不利因素。此外,口服甲氨蝶呤消除了注射的需要,这对年幼的儿童尤其重要。有必要对儿童和青少年患者进行对照、随机前瞻性试验,以明确推荐甲氨蝶呤皮下给药途径。


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


