Anabel Franco-Moreno, David Brown-Lavalle, Nicolás Rodríguez-Ramírez, Candela Muñoz-Roldán, Ana Ignes Rubio-Aguilera, Maria Campos-Arenas, Nuria Muñoz-Rivas, Eva Moya-Mateo, José Manuel Ruiz-Giardín, Virginia Pardo-Guimerá, Mariano Ulla-Anes, Roberto Pedrero-Tomé, Juan Torres-Macho, Ana Bustamante-Fermosel
{"title":"Clinical prediction model for pulmonary thrombosis diagnosis in hospitalized patients with SARS-CoV-2 infection.","authors":"Anabel Franco-Moreno, David Brown-Lavalle, Nicolás Rodríguez-Ramírez, Candela Muñoz-Roldán, Ana Ignes Rubio-Aguilera, Maria Campos-Arenas, Nuria Muñoz-Rivas, Eva Moya-Mateo, José Manuel Ruiz-Giardín, Virginia Pardo-Guimerá, Mariano Ulla-Anes, Roberto Pedrero-Tomé, Juan Torres-Macho, Ana Bustamante-Fermosel","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aim: </strong>We aimed to develop a clinical prediction model for pulmonary thrombosis (PT) diagnosis in hospitalized COVID-19 patients.</p><p><strong>Methods: </strong>Non-intensive care unit hospitalized COVID-19 patients who underwent a computed tomography pulmonary angiogram (CTPA) for suspected PT were included in the study. Demographic, clinical, analytical, and radiological variables as potential factors associated with the presence of PT were selected. Multivariable Cox regression analysis to develop a score for estimating the pre-test probability of PT was performed. The score was internally validated by bootstrap analysis.</p><p><strong>Results: </strong>Among the 271 patients who underwent a CTPA, 132 patients (48.7%) had PT. Heart rate >100 bpm (OR = 4.63 [95% CI: 2.30-9.34]; <i>P</i> < 0.001), respiratory rate >22 bpm (OR = 5.21 [95% CI: 2.00-13.54]; <i>P</i> < 0.001), RALE score ≥4 (OR = 3.24 [95% CI: 1.66-6.32]; <i>P</i> < 0.001), C-reactive protein (CRP) >100 mg/L (OR = 2.10 [95% CI: 0.95-4.63]; <i>P</i> = 0.067), and D-dimer >3.000 ng/mL (OR = 6.86 [95% CI: 3.54-13.28]; <i>P</i> < 0.001) at the time of suspected PT were independent predictors of thrombosis. Using these variables, we constructed a nomogram (CRP, Heart rate, D-dimer, RALE score, and respiratory rate [CHEDDAR score]) for estimating the pre-test probability of PT. The score showed a high predictive accuracy (area under the receiver-operating characteristics curve = 0.877; 95% CI: 0.83-0.92). A score lower than 182 points on the nomogram confers a low probability for PT with a negative predictive value of 92%.</p><p><strong>Conclusions: </strong>CHEDDAR score can be used to estimate the pre-test probability of PT in hospitalized COVID-19 patients outside the intensive care unit.</p><p><strong>Relevance for patients: </strong>Developing a new clinical prediction model for PT diagnosis in COVID-19 may help in the triage of patients, and limit unnecessary exposure to radiation and the risk of nephrotoxicity due to iodinated contrast.</p>","PeriodicalId":15482,"journal":{"name":"Journal of Clinical and Translational Research","volume":"9 2","pages":"59-68"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/33/37/jclintranslres-2023-9-2-59.PMC10075091.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Translational Research","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aim: We aimed to develop a clinical prediction model for pulmonary thrombosis (PT) diagnosis in hospitalized COVID-19 patients.
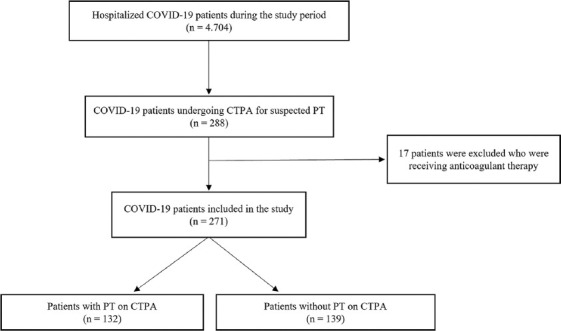
Methods: Non-intensive care unit hospitalized COVID-19 patients who underwent a computed tomography pulmonary angiogram (CTPA) for suspected PT were included in the study. Demographic, clinical, analytical, and radiological variables as potential factors associated with the presence of PT were selected. Multivariable Cox regression analysis to develop a score for estimating the pre-test probability of PT was performed. The score was internally validated by bootstrap analysis.
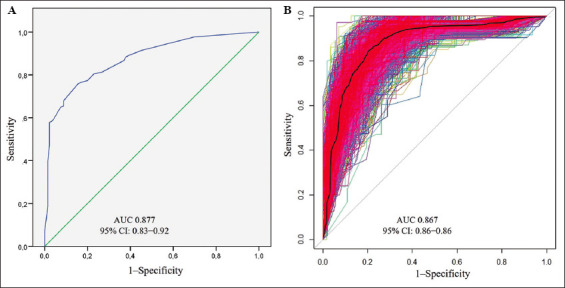
Results: Among the 271 patients who underwent a CTPA, 132 patients (48.7%) had PT. Heart rate >100 bpm (OR = 4.63 [95% CI: 2.30-9.34]; P < 0.001), respiratory rate >22 bpm (OR = 5.21 [95% CI: 2.00-13.54]; P < 0.001), RALE score ≥4 (OR = 3.24 [95% CI: 1.66-6.32]; P < 0.001), C-reactive protein (CRP) >100 mg/L (OR = 2.10 [95% CI: 0.95-4.63]; P = 0.067), and D-dimer >3.000 ng/mL (OR = 6.86 [95% CI: 3.54-13.28]; P < 0.001) at the time of suspected PT were independent predictors of thrombosis. Using these variables, we constructed a nomogram (CRP, Heart rate, D-dimer, RALE score, and respiratory rate [CHEDDAR score]) for estimating the pre-test probability of PT. The score showed a high predictive accuracy (area under the receiver-operating characteristics curve = 0.877; 95% CI: 0.83-0.92). A score lower than 182 points on the nomogram confers a low probability for PT with a negative predictive value of 92%.
Conclusions: CHEDDAR score can be used to estimate the pre-test probability of PT in hospitalized COVID-19 patients outside the intensive care unit.
Relevance for patients: Developing a new clinical prediction model for PT diagnosis in COVID-19 may help in the triage of patients, and limit unnecessary exposure to radiation and the risk of nephrotoxicity due to iodinated contrast.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


