{"title":"Medium-Term Risk of Recurrent Pelvic Organ Prolapse within 2-Year Follow-Up after Laparoscopic Sacrocolpopexy.","authors":"Hirotaka Sato, Shota Otsuka, Hirokazu Abe, Tomoaki Miyagawa","doi":"10.4103/gmit.gmit_59_22","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The present study was performed to determine the risk of recurrent pelvic organ prolapse (POP) within 2 years after laparoscopic sacrocolpopexy (LSC) in patients with uterovaginal prolapse.</p><p><strong>Materials and methods: </strong>A retrospective comparative study was performed in a population of 204 patients over a 2-year follow-up period following LSC with concomitant supracervical hysterectomy or uterine preservation at a single urological clinic between 2015 and 2019. The primary outcome was surgical failure following LSC in cases of POP, focusing on failures occurring before the 2<sup>nd</sup>year of follow-up. Logistic regression analysis was used to determine the odds ratios (ORs) for surgical failure.</p><p><strong>Results: </strong>The primary outcome, surgical failure in cases of POP, occurred 2 years after the initial surgery in 19 of the 204 patients (9.3%) (95% confidence interval [CI], 5.7% - 14.2%). Surgical failure was most common in the anterior compartment (<i>n</i> = 10, 4.9%), and further surgery was performed in seven of the patients with surgical failure (3.4%). The poor primary outcome was predicted by lysis of adhesions (OR, 7.5, 95% CI, 1.6-33.8, <i>P</i> = 0.008) and preoperative POP stage IV (OR, 3.5; 95% CI, 1.1-10.8, <i>P</i> = 0.03) on multivariable logistic regression analysis.</p><p><strong>Conclusion: </strong>The overall rate of surgical failure following LSC in our cohort was 9.3% over the 2-year follow-up period after surgery, and preoperative prolapse stage IV was associated with a higher risk of recurrence.</p>","PeriodicalId":45272,"journal":{"name":"Gynecology and Minimally Invasive Therapy-GMIT","volume":"12 1","pages":"38-43"},"PeriodicalIF":1.4000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/91/2a/GMIT-12-38.PMC10071876.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gynecology and Minimally Invasive Therapy-GMIT","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/gmit.gmit_59_22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The present study was performed to determine the risk of recurrent pelvic organ prolapse (POP) within 2 years after laparoscopic sacrocolpopexy (LSC) in patients with uterovaginal prolapse.
Materials and methods: A retrospective comparative study was performed in a population of 204 patients over a 2-year follow-up period following LSC with concomitant supracervical hysterectomy or uterine preservation at a single urological clinic between 2015 and 2019. The primary outcome was surgical failure following LSC in cases of POP, focusing on failures occurring before the 2ndyear of follow-up. Logistic regression analysis was used to determine the odds ratios (ORs) for surgical failure.
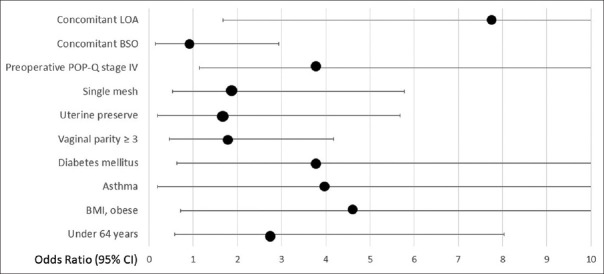
Results: The primary outcome, surgical failure in cases of POP, occurred 2 years after the initial surgery in 19 of the 204 patients (9.3%) (95% confidence interval [CI], 5.7% - 14.2%). Surgical failure was most common in the anterior compartment (n = 10, 4.9%), and further surgery was performed in seven of the patients with surgical failure (3.4%). The poor primary outcome was predicted by lysis of adhesions (OR, 7.5, 95% CI, 1.6-33.8, P = 0.008) and preoperative POP stage IV (OR, 3.5; 95% CI, 1.1-10.8, P = 0.03) on multivariable logistic regression analysis.
Conclusion: The overall rate of surgical failure following LSC in our cohort was 9.3% over the 2-year follow-up period after surgery, and preoperative prolapse stage IV was associated with a higher risk of recurrence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


