Validation of a preoperative formula to estimate postoperative pelvic sagittal alignment and mobility before performing total hip arthroplasty for patients with hip osteoarthritis.
{"title":"Validation of a preoperative formula to estimate postoperative pelvic sagittal alignment and mobility before performing total hip arthroplasty for patients with hip osteoarthritis.","authors":"Hiroki Tanabe, Yasuhiro Homma, Naotake Yanagisawa, Taiji Watari, Seiya Ishii, Yuichi Shirogane, Tomonori Baba, Kazuo Kaneko, Muneaki Ishijima","doi":"10.1186/s42836-023-00171-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although it is important to consider pelvic alignment and mobility in the standing and sitting positions before THA, it is not known how to preoperatively predict individual postoperative pelvic alignment and mobility. The purpose of this study was to investigate the pelvic alignment and mobility before and after THA, and to develop a predictive formula using preoperative factors to calculate postoperative sagittal alignment and mobility.</p><p><strong>Methods: </strong>One hundred seventy patients were assessed. The 170 patients were randomly divided into a prediction model analysis group (n = 85) and an external validation group (n = 85). In the prediction model analysis group, preoperative spinopelvic parameters were used to develop the predictive formulas to predict the postoperative sacral slope (SS) in standing and sitting positions and ΔSS. These were applied to the external validation group and assessed.</p><p><strong>Results: </strong>R<sup>2</sup> in multiple linear regression models for postoperative SS in standing, SS in sitting and ΔSS were 0.810, 0.672, and 0.423, respectively. The values of predicted and postoperative parameters were very close with no significant difference: SS in standing (33.87 vs. 34.23, P = 0.834), SS in sitting (18.86 vs. 19.51, P = 0.228), and ΔSS (15.38 vs. 14.72, P = 0.619).</p><p><strong>Conclusion: </strong>The present study showed that the pelvic alignment and mobility after THA can be predicted using preoperative factors. Although a model with higher accuracy is needed, it is important to use a predictive formula to estimate the postoperative condition before performing THA.</p>","PeriodicalId":52831,"journal":{"name":"Arthroplasty","volume":null,"pages":null},"PeriodicalIF":2.3000,"publicationDate":"2023-04-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10077599/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arthroplasty","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s42836-023-00171-w","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Although it is important to consider pelvic alignment and mobility in the standing and sitting positions before THA, it is not known how to preoperatively predict individual postoperative pelvic alignment and mobility. The purpose of this study was to investigate the pelvic alignment and mobility before and after THA, and to develop a predictive formula using preoperative factors to calculate postoperative sagittal alignment and mobility.
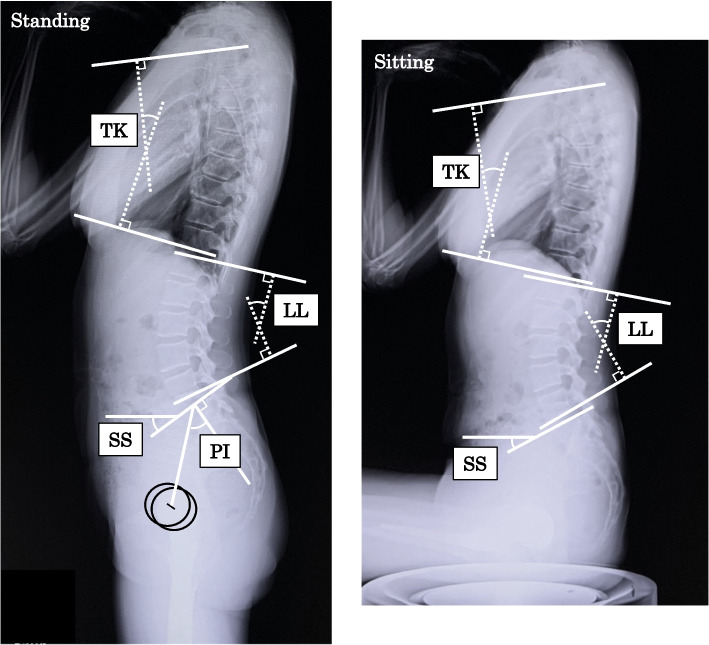
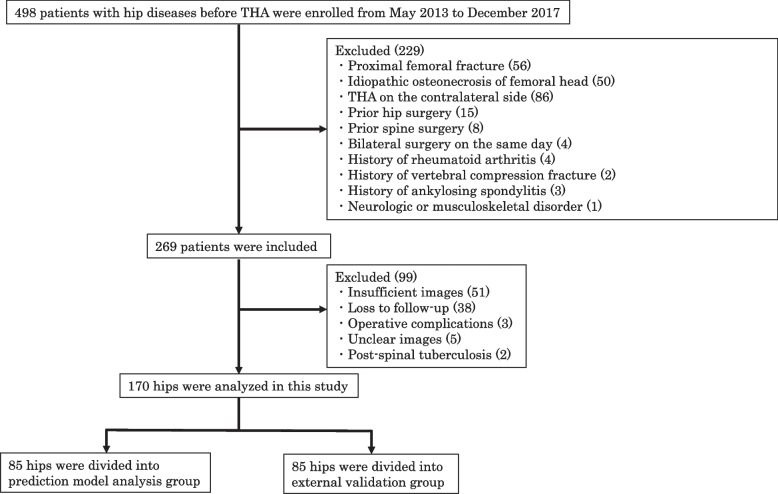
Methods: One hundred seventy patients were assessed. The 170 patients were randomly divided into a prediction model analysis group (n = 85) and an external validation group (n = 85). In the prediction model analysis group, preoperative spinopelvic parameters were used to develop the predictive formulas to predict the postoperative sacral slope (SS) in standing and sitting positions and ΔSS. These were applied to the external validation group and assessed.
Results: R2 in multiple linear regression models for postoperative SS in standing, SS in sitting and ΔSS were 0.810, 0.672, and 0.423, respectively. The values of predicted and postoperative parameters were very close with no significant difference: SS in standing (33.87 vs. 34.23, P = 0.834), SS in sitting (18.86 vs. 19.51, P = 0.228), and ΔSS (15.38 vs. 14.72, P = 0.619).
Conclusion: The present study showed that the pelvic alignment and mobility after THA can be predicted using preoperative factors. Although a model with higher accuracy is needed, it is important to use a predictive formula to estimate the postoperative condition before performing THA.
背景:尽管在全髋关节置换术前考虑站立和坐姿的骨盆对准和活动是很重要的,但术前如何预测个体术后骨盆对准和活动尚不清楚。本研究的目的是研究髋关节置换术前后的骨盆对准度和活动性,并利用术前因素建立一个预测公式来计算术后矢状位对准度和活动性。方法:对170例患者进行评估。170例患者随机分为预测模型分析组(n = 85)和外部验证组(n = 85)。预测模型分析组采用术前脊柱骨盆参数建立预测公式,预测术后站位、坐位及ΔSS的骶骨斜率(SS)。将这些应用于外部验证组并进行评估。结果:术后站立SS、坐位SS和ΔSS的多元线性回归模型R2分别为0.810、0.672、0.423。预测值与术后参数非常接近,无显著差异:站立时SS (33.87 vs. 34.23, P = 0.834),坐位时SS (18.86 vs. 19.51, P = 0.228), ΔSS (15.38 vs. 14.72, P = 0.619)。结论:本研究表明,术前因素可以预测THA术后骨盆的排列和活动。虽然需要更高精度的模型,但在进行THA手术前,使用预测公式来估计术后情况是很重要的。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


