{"title":"Overlapping clinical features of systemic juvenile idiopathic arthritis and SARS-CoV-2-related multisystem inflammatory syndrome in children.","authors":"Oksana Boyarchuk, Tetiana Kovalchuk","doi":"10.5114/reum/161185","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Differential diagnosis of the systemic juvenile idiopathic arthritis (sJIA) is often complicated, because of the variability in clinical presentation and the absence of specific signs.</p><p><strong>Material and methods: </strong>The PubMed/Medline and Scopus databases from the years 2013-2022 were analysed for full articles in English and the following key words were used: \"juvenile idiopathic arthritis\" and \"MIS-C\"; \"juvenile idiopathic arthritis\" and \"Kawasaki disease\". As an example of the problem the case description of a 3-year-old patient is presented.</p><p><strong>Results: </strong>In the first step 167 publications were identified; however, after exclusion of duplicated articles and those not relevant to the topic, only 13 were included in the analysis. We analysed studies that describe overlapping clinical features of sJIA and Kawasaki disease (KD) or multisystem inflammatory syndrome in children (MIS-C). The main issues we discussed were the search for the specific features that would distinguish one disease from another. Fever refractory to intravenous immunoglobulin treatment was the most frequent indicator among the features of clinical courses. Among other clinical signs prolonged, recurrent fever, rash, an incomplete KD phenotype, Caucasian race, splenomegaly, and complicated macrophage activation syndrome also supported sJIA diagnosis. Among laboratory tests, high ferritin and serum interleukin-18 levels were found to be the most useful in differentiation. The present case demonstrates that prolonged, unexplained, recurrent fever with a specific pattern should be the reason to suspect sJIA.</p><p><strong>Conclusions: </strong>Overlapping features of sJIA and SARS-CoV-2-related MIS-C complicates diagnosis in the era of the COVID-19 pandemic. Our case presentation adds symptoms of prolonged, spiking, unexplained, recurrent fever with a specific pattern for supporting systemic juvenile idiopathic arthritis diagnosis.</p>","PeriodicalId":21312,"journal":{"name":"Reumatologia","volume":"61 1","pages":"63-70"},"PeriodicalIF":1.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6e/30/RU-61-161185.PMC10044031.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reumatologia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/reum/161185","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 2
Abstract
Introduction: Differential diagnosis of the systemic juvenile idiopathic arthritis (sJIA) is often complicated, because of the variability in clinical presentation and the absence of specific signs.
Material and methods: The PubMed/Medline and Scopus databases from the years 2013-2022 were analysed for full articles in English and the following key words were used: "juvenile idiopathic arthritis" and "MIS-C"; "juvenile idiopathic arthritis" and "Kawasaki disease". As an example of the problem the case description of a 3-year-old patient is presented.
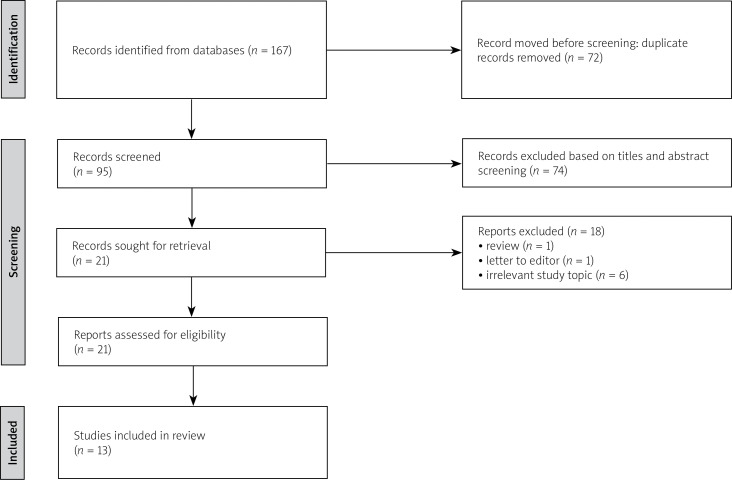
Results: In the first step 167 publications were identified; however, after exclusion of duplicated articles and those not relevant to the topic, only 13 were included in the analysis. We analysed studies that describe overlapping clinical features of sJIA and Kawasaki disease (KD) or multisystem inflammatory syndrome in children (MIS-C). The main issues we discussed were the search for the specific features that would distinguish one disease from another. Fever refractory to intravenous immunoglobulin treatment was the most frequent indicator among the features of clinical courses. Among other clinical signs prolonged, recurrent fever, rash, an incomplete KD phenotype, Caucasian race, splenomegaly, and complicated macrophage activation syndrome also supported sJIA diagnosis. Among laboratory tests, high ferritin and serum interleukin-18 levels were found to be the most useful in differentiation. The present case demonstrates that prolonged, unexplained, recurrent fever with a specific pattern should be the reason to suspect sJIA.
Conclusions: Overlapping features of sJIA and SARS-CoV-2-related MIS-C complicates diagnosis in the era of the COVID-19 pandemic. Our case presentation adds symptoms of prolonged, spiking, unexplained, recurrent fever with a specific pattern for supporting systemic juvenile idiopathic arthritis diagnosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


