Andrew Nguyen, Akshay Reddy, Ramy Sharaf, Lauren Ladehoff, Michael Joseph Diaz, Brandon Lucke-Wold
{"title":"Outcomes of surgical management and implant consideration for depressed skull fractures: A systematic review.","authors":"Andrew Nguyen, Akshay Reddy, Ramy Sharaf, Lauren Ladehoff, Michael Joseph Diaz, Brandon Lucke-Wold","doi":"10.36922/an.247","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Traumatic brain injuries (TBIs) are associated with high mortality and morbidity. Depressed skull fractures (DSFs) are a subset of fractures characterized by either direct or indirect brain damage, compressing brain tissue. Recent advances in implant use during primary reconstruction surgeries have shown to be effective. In this systematic review, we assess differences in titanium mesh, polyetheretherketone (PEEK) implants, autologous pericranial grafts, and methyl methacrylate (PMMA) implants for DSF treatment.</p><p><strong>Methods: </strong>A literature search was conducted in PubMed, Scopus, and Web of Science from their inception to September 2022 to retrieve articles regarding the use of various implant materials for depressed skull fractures. Inclusion criteria included studies specifically describing implant type/material within treatment of depressed skull fractures, particularly during duraplasty. Exclusion criteria were studies reporting only non-primary data, those insufficiently disaggregated to extract implant type, those describing treatment of pathologies other than depressed skull fractures, and non-English or cadaveric studies. The Newcastle-Ottawa Scale was utilized to assess for presence of bias in included studies.</p><p><strong>Results: </strong>Following final study selection, 18 articles were included for quantitative and qualitative analysis. Of the 177 patients (152 males), mean age was 30.8 years with 82% implanted with autologous graft material, and 18% with non-autologous material. Data were pooled and analyzed with respect to the total patient set, and additionally stratified into those treated through autologous and non-autologous implant material.There were no differences between the two cohorts regarding mean time to encounter, pre-operative Glasgow coma scale (GCS), fracture location, length to cranioplasty, and complication rate. There were statistically significant differences in post-operative GCS (p < 0.0001), LOS (p = 0.0274), and minimum follow-up time (p = 0.000796).</p><p><strong>Conclusion: </strong>Differences in measurable post-operative outcomes between implant groups were largely minimal or none. Future research should aim to probe these basic results deeper with a larger, non-biased sample.</p>","PeriodicalId":72072,"journal":{"name":"Advanced neurology","volume":"2 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-03-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advanced neurology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36922/an.247","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/2/3 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Traumatic brain injuries (TBIs) are associated with high mortality and morbidity. Depressed skull fractures (DSFs) are a subset of fractures characterized by either direct or indirect brain damage, compressing brain tissue. Recent advances in implant use during primary reconstruction surgeries have shown to be effective. In this systematic review, we assess differences in titanium mesh, polyetheretherketone (PEEK) implants, autologous pericranial grafts, and methyl methacrylate (PMMA) implants for DSF treatment.
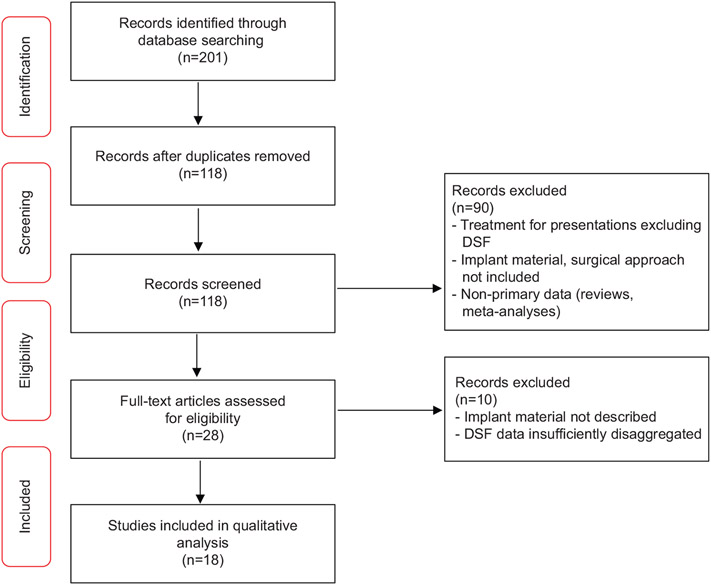
Methods: A literature search was conducted in PubMed, Scopus, and Web of Science from their inception to September 2022 to retrieve articles regarding the use of various implant materials for depressed skull fractures. Inclusion criteria included studies specifically describing implant type/material within treatment of depressed skull fractures, particularly during duraplasty. Exclusion criteria were studies reporting only non-primary data, those insufficiently disaggregated to extract implant type, those describing treatment of pathologies other than depressed skull fractures, and non-English or cadaveric studies. The Newcastle-Ottawa Scale was utilized to assess for presence of bias in included studies.
Results: Following final study selection, 18 articles were included for quantitative and qualitative analysis. Of the 177 patients (152 males), mean age was 30.8 years with 82% implanted with autologous graft material, and 18% with non-autologous material. Data were pooled and analyzed with respect to the total patient set, and additionally stratified into those treated through autologous and non-autologous implant material.There were no differences between the two cohorts regarding mean time to encounter, pre-operative Glasgow coma scale (GCS), fracture location, length to cranioplasty, and complication rate. There were statistically significant differences in post-operative GCS (p < 0.0001), LOS (p = 0.0274), and minimum follow-up time (p = 0.000796).
Conclusion: Differences in measurable post-operative outcomes between implant groups were largely minimal or none. Future research should aim to probe these basic results deeper with a larger, non-biased sample.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


