Shyam Patel, Chelsea Alfafara, Molly B Kraus, Skye Buckner-Petty, Timethia Bonner, Mohanad R Youssef, Karl A Poterack, Girish Mour, Amit K Mathur, Adam J Milam
{"title":"Individual- and Community-Level Socioeconomic Status and Deceased Donor Renal Transplant Outcomes.","authors":"Shyam Patel, Chelsea Alfafara, Molly B Kraus, Skye Buckner-Petty, Timethia Bonner, Mohanad R Youssef, Karl A Poterack, Girish Mour, Amit K Mathur, Adam J Milam","doi":"10.1007/s40615-023-01851-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study examined the relationship between socioeconomic status (SES), race, and ethnicity and clinical outcomes following deceased donor kidney transplant (DDKT) at a high-volume transplant center.</p><p><strong>Methods: </strong>This retrospective cohort study used regression models and survival analyses to examine the relationship between individual- and community-level SES, race, and ethnicity and DDKT outcomes (i.e., delayed graft function, graft failure, mortality) adjusting for potential confounders.</p><p><strong>Results: </strong>The analytic sample included 3366 patients; 40.7% (n = 1370) were female, the mean age was 54.7 (SD = 13.3) years, 49.3% were non-Hispanic White, and the median follow-up time was 39.5 months (IQR = 24.2-68.1). Patients living in the most disadvantaged communities (using the US Census data) had a higher likelihood of delayed graft function (adjusted relative risk [RR] = 1.12, p = 0.042) and a higher hazard of mortality (adjusted hazard ratio [HR] = 1.32, p = 0.025) compared to patients living in the least disadvantaged communities. Patients without a high school diploma had a higher risk of delayed graft function compared to patients with an associate degree or more (RR = 1.37, p < 0.001). Patients with public insurance coverage had a higher risk of delayed graft function (RR = 1.24, p < 0.001) and a higher hazard of mortality (HR = 1.37, p < 0.001) and graft failure (HR = 1.71, p < 0.001) compared to patients without public insurance. There were no differences in graft failure or mortality by race and ethnicity.</p><p><strong>Conclusions: </strong>SES was not consistently associated with outcomes following DDKT; however, many of the predictors were associated with delayed graft function. With a large and diverse sample size, these findings further the heterogeneity of the present renal transplant research suggesting the need for further investigation to guide implementation of innovative strategies and interventions.</p>","PeriodicalId":16921,"journal":{"name":"Journal of Racial and Ethnic Health Disparities","volume":" ","pages":"68-78"},"PeriodicalIF":3.2000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Racial and Ethnic Health Disparities","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40615-023-01851-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/14 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This study examined the relationship between socioeconomic status (SES), race, and ethnicity and clinical outcomes following deceased donor kidney transplant (DDKT) at a high-volume transplant center.
Methods: This retrospective cohort study used regression models and survival analyses to examine the relationship between individual- and community-level SES, race, and ethnicity and DDKT outcomes (i.e., delayed graft function, graft failure, mortality) adjusting for potential confounders.
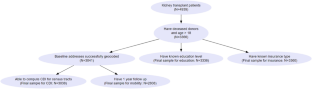
Results: The analytic sample included 3366 patients; 40.7% (n = 1370) were female, the mean age was 54.7 (SD = 13.3) years, 49.3% were non-Hispanic White, and the median follow-up time was 39.5 months (IQR = 24.2-68.1). Patients living in the most disadvantaged communities (using the US Census data) had a higher likelihood of delayed graft function (adjusted relative risk [RR] = 1.12, p = 0.042) and a higher hazard of mortality (adjusted hazard ratio [HR] = 1.32, p = 0.025) compared to patients living in the least disadvantaged communities. Patients without a high school diploma had a higher risk of delayed graft function compared to patients with an associate degree or more (RR = 1.37, p < 0.001). Patients with public insurance coverage had a higher risk of delayed graft function (RR = 1.24, p < 0.001) and a higher hazard of mortality (HR = 1.37, p < 0.001) and graft failure (HR = 1.71, p < 0.001) compared to patients without public insurance. There were no differences in graft failure or mortality by race and ethnicity.
Conclusions: SES was not consistently associated with outcomes following DDKT; however, many of the predictors were associated with delayed graft function. With a large and diverse sample size, these findings further the heterogeneity of the present renal transplant research suggesting the need for further investigation to guide implementation of innovative strategies and interventions.
期刊介绍:
Journal of Racial and Ethnic Health Disparities reports on the scholarly progress of work to understand, address, and ultimately eliminate health disparities based on race and ethnicity. Efforts to explore underlying causes of health disparities and to describe interventions that have been undertaken to address racial and ethnic health disparities are featured. Promising studies that are ongoing or studies that have longer term data are welcome, as are studies that serve as lessons for best practices in eliminating health disparities. Original research, systematic reviews, and commentaries presenting the state-of-the-art thinking on problems centered on health disparities will be considered for publication. We particularly encourage review articles that generate innovative and testable ideas, and constructive discussions and/or critiques of health disparities.Because the Journal of Racial and Ethnic Health Disparities receives a large number of submissions, about 30% of submissions to the Journal are sent out for full peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


