Calcedonio Calcara, Sila Cocciolillo, Ylenia Marten Canavesio, Vincenzo Adamo, Silvia Carenzi, Daria Ilenia Lucci, Alberto Premoli
{"title":"Endoscopic fluorescent lymphography for gastric cancer.","authors":"Calcedonio Calcara, Sila Cocciolillo, Ylenia Marten Canavesio, Vincenzo Adamo, Silvia Carenzi, Daria Ilenia Lucci, Alberto Premoli","doi":"10.4253/wjge.v15.i2.32","DOIUrl":null,"url":null,"abstract":"<p><p>Lymphography by radioisotope or dye is a well-known technique for visualizing the lymphatic drainage pattern in a neoplastic lesion and it is in use in gastric cancer. Indocyanine green (ICG) more recently has been validated in fluorescent lymphography studies and is under evaluation as a novel tracer agent in gastric cancer. The amount and dilution of ICG injected as well as the site and the time of the injection are not standardized. In our unit, endoscopic submucosal injections of ICG are made as 0.5 mg in 0.5 mL at four peritumoral sites the day before surgery (for a total of 2.0 mg in 2.0 mL). Detection instruments for ICG fluorescence are evolving. Near-infrared systems integrated into laparoscopic or robotic instruments (near-infrared fluorescence imaging) have shown the most promising results. ICG fluorescence recognizes the node that receives lymphatic flow directly from a primary tumor. This is defined as the sentinel lymph node, and it has a high predictive negative value at the cT1 stage, able to reduce the extent of gastrectomy and lymph node dissection. ICG also enhances the number of lymph nodes detected during extended lymphadenectomy for advanced gastric cancer. Nevertheless, the practical effects of ICG use in a single patient are not yet clear. Standardization of the technique and further studies are needed before fluorescent lymphography can be used extensively worldwide. Until then, current guidelines recommend an extensive lymphadenectomy as the standard approach for gastric cancer with suspected metastasis.</p>","PeriodicalId":23953,"journal":{"name":"World Journal of Gastrointestinal Endoscopy","volume":"15 2","pages":"32-43"},"PeriodicalIF":1.4000,"publicationDate":"2023-02-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/38/fb/WJGE-15-32.PMC10011894.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4253/wjge.v15.i2.32","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
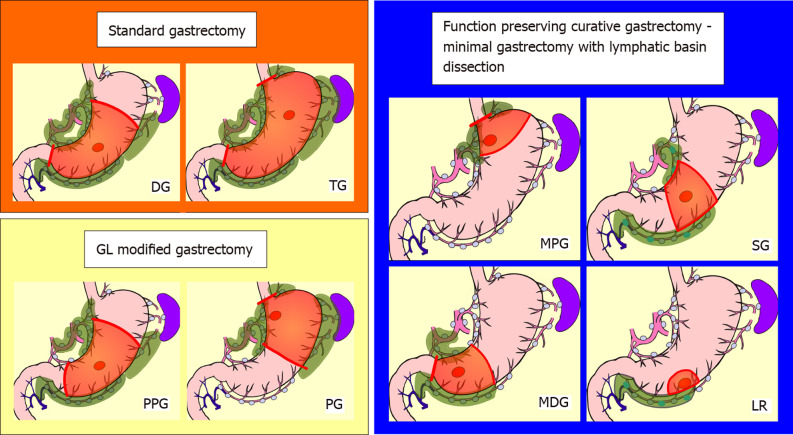
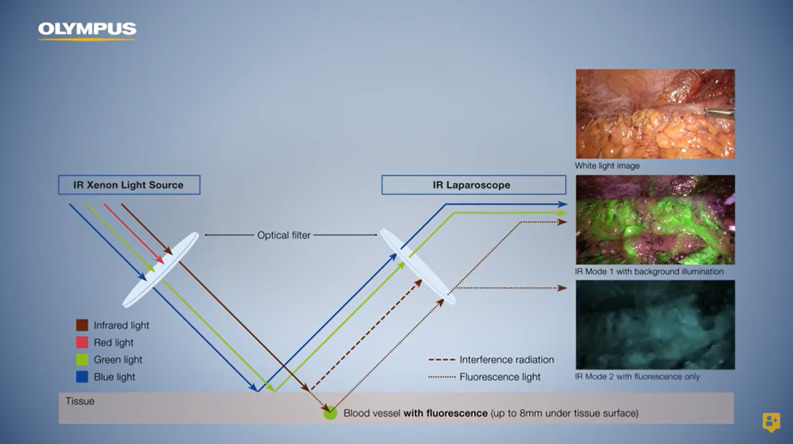
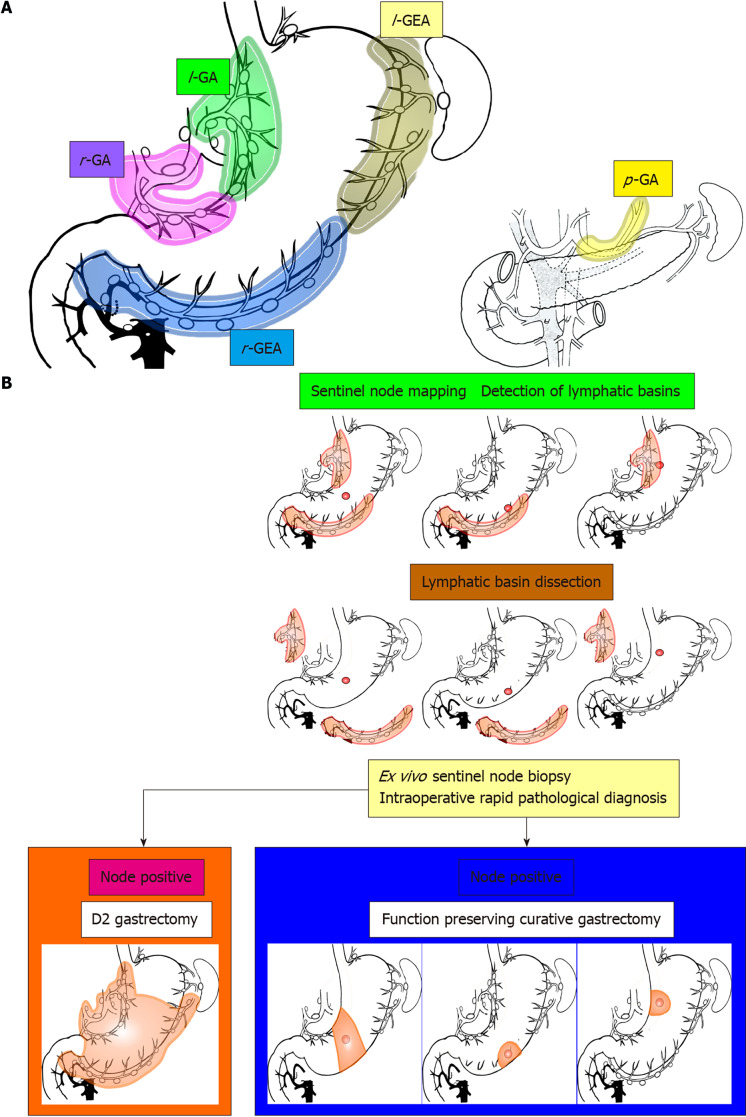
Lymphography by radioisotope or dye is a well-known technique for visualizing the lymphatic drainage pattern in a neoplastic lesion and it is in use in gastric cancer. Indocyanine green (ICG) more recently has been validated in fluorescent lymphography studies and is under evaluation as a novel tracer agent in gastric cancer. The amount and dilution of ICG injected as well as the site and the time of the injection are not standardized. In our unit, endoscopic submucosal injections of ICG are made as 0.5 mg in 0.5 mL at four peritumoral sites the day before surgery (for a total of 2.0 mg in 2.0 mL). Detection instruments for ICG fluorescence are evolving. Near-infrared systems integrated into laparoscopic or robotic instruments (near-infrared fluorescence imaging) have shown the most promising results. ICG fluorescence recognizes the node that receives lymphatic flow directly from a primary tumor. This is defined as the sentinel lymph node, and it has a high predictive negative value at the cT1 stage, able to reduce the extent of gastrectomy and lymph node dissection. ICG also enhances the number of lymph nodes detected during extended lymphadenectomy for advanced gastric cancer. Nevertheless, the practical effects of ICG use in a single patient are not yet clear. Standardization of the technique and further studies are needed before fluorescent lymphography can be used extensively worldwide. Until then, current guidelines recommend an extensive lymphadenectomy as the standard approach for gastric cancer with suspected metastasis.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


