The Impact of Complete Revascularization in Symptomatic Severe Left Ventricular Dysfunction between Coronary Artery Bypass Graft and Percutaneous Coronary Intervention.
Hsiu-Yu Fang, Yen-Nan Fang, Yin-Chia Chen, Jiunn-Jye Sheu, Wei-Chieh Lee
{"title":"The Impact of Complete Revascularization in Symptomatic Severe Left Ventricular Dysfunction between Coronary Artery Bypass Graft and Percutaneous Coronary Intervention.","authors":"Hsiu-Yu Fang, Yen-Nan Fang, Yin-Chia Chen, Jiunn-Jye Sheu, Wei-Chieh Lee","doi":"10.1155/2023/9226722","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The study aimed to compare the clinical outcomes between the patients receiving coronary artery bypass surgery (CABG) or percutaneous coronary intervention (PCI) for the patients with symptomatic severe left ventricular (LV) dysfunction and coronary artery disease (CAD).</p><p><strong>Methods: </strong>Between February 2007 and February 2020, a total of 745 patients who received coronary artery angiography for reduced LV ejection fraction (LVEF) < 40% and symptomatic New York Heart Association (NYHA) functional class ≥ 3 were recruited. The patients (<i>N</i> = 236) who were diagnosed with dilated cardiomyopathy or valvular heart disease without coronary artery stenosis, those with prior history of CABG or valvular surgery (<i>N</i> = 59), those who presented ST-segment elevated myocardial infarction (STEMI), those with a CAD and SYNTAX score of ≦ 22 (<i>N</i> = 175), those who received emergent CABG for coronary perforation (<i>N</i> = 3), and those who had NYHA class ≦ 2 (<i>N</i> = 65) were excluded. Finally, 116 patients with reduced LVEF and those who had a SYNTAX score >22, who received CABG (N = 47) and PCI (N = 69), were recruited for this study.</p><p><strong>Results: </strong>There was no significant difference in the incidence values of in-hospital course and those of in-hospital mortality, acute kidney injury, and postprocedural hemodialysis. There was no significant difference in the 1-yearfollow-up of recurrent MI, revascularization, or stroke between the groups. The 1-year heart failure (HF) hospitalization rate was significantly lower in the CABG group than in all patients of the PCI group (13.2% vs. 33.3%; <i>p</i> = 0.035); however, there was no significant difference in the same variable between the CABG group and the complete revascularization subgroup (13.2% vs. 28.2%; <i>p</i> = 0.160). The revascularization index (RI) was significantly higher in the CABG group than in all patients of the PCI group or complete revascularization subgroup (0.93 ± 0.12 vs. 0.71 ± 0.25; <i>p</i> < 0.001) and (0.93 ± 0.12 vs. 0.86 ± 0.13; <i>p</i> = 0.019). The 3-year HF hospitalization rate was significantly lower in the CABG group than in all patients of the PCI group (16.2% vs. 42.2%; <i>p</i> = 0.008); however, there was no difference in the same variable between the CABG group and the complete revascularization subgroup (16.2% vs. 35.1%; <i>p</i> = 0.109).</p><p><strong>Conclusions: </strong>In patients with symptomatic (NYHA class ≥ 3) severe LV dysfunction and CAD, CABG brought less HF admission when compared to patients in the PCI group, but this did not differ when compared to the complete revascularization subgroup. Therefore, an extensive revascularization, achieved by CABG or PCI, is associated with a lower HF hospitalization rate during the 3-yearfollow-up period in such populations.</p>","PeriodicalId":9494,"journal":{"name":"Cardiology Research and Practice","volume":"2023 ","pages":"9226722"},"PeriodicalIF":1.8000,"publicationDate":"2023-02-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9991473/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research and Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2023/9226722","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The study aimed to compare the clinical outcomes between the patients receiving coronary artery bypass surgery (CABG) or percutaneous coronary intervention (PCI) for the patients with symptomatic severe left ventricular (LV) dysfunction and coronary artery disease (CAD).
Methods: Between February 2007 and February 2020, a total of 745 patients who received coronary artery angiography for reduced LV ejection fraction (LVEF) < 40% and symptomatic New York Heart Association (NYHA) functional class ≥ 3 were recruited. The patients (N = 236) who were diagnosed with dilated cardiomyopathy or valvular heart disease without coronary artery stenosis, those with prior history of CABG or valvular surgery (N = 59), those who presented ST-segment elevated myocardial infarction (STEMI), those with a CAD and SYNTAX score of ≦ 22 (N = 175), those who received emergent CABG for coronary perforation (N = 3), and those who had NYHA class ≦ 2 (N = 65) were excluded. Finally, 116 patients with reduced LVEF and those who had a SYNTAX score >22, who received CABG (N = 47) and PCI (N = 69), were recruited for this study.
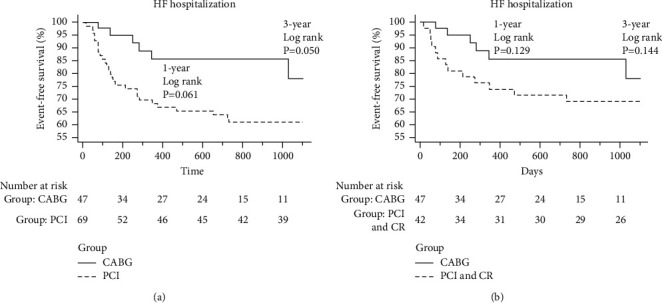
Results: There was no significant difference in the incidence values of in-hospital course and those of in-hospital mortality, acute kidney injury, and postprocedural hemodialysis. There was no significant difference in the 1-yearfollow-up of recurrent MI, revascularization, or stroke between the groups. The 1-year heart failure (HF) hospitalization rate was significantly lower in the CABG group than in all patients of the PCI group (13.2% vs. 33.3%; p = 0.035); however, there was no significant difference in the same variable between the CABG group and the complete revascularization subgroup (13.2% vs. 28.2%; p = 0.160). The revascularization index (RI) was significantly higher in the CABG group than in all patients of the PCI group or complete revascularization subgroup (0.93 ± 0.12 vs. 0.71 ± 0.25; p < 0.001) and (0.93 ± 0.12 vs. 0.86 ± 0.13; p = 0.019). The 3-year HF hospitalization rate was significantly lower in the CABG group than in all patients of the PCI group (16.2% vs. 42.2%; p = 0.008); however, there was no difference in the same variable between the CABG group and the complete revascularization subgroup (16.2% vs. 35.1%; p = 0.109).
Conclusions: In patients with symptomatic (NYHA class ≥ 3) severe LV dysfunction and CAD, CABG brought less HF admission when compared to patients in the PCI group, but this did not differ when compared to the complete revascularization subgroup. Therefore, an extensive revascularization, achieved by CABG or PCI, is associated with a lower HF hospitalization rate during the 3-yearfollow-up period in such populations.
研究目的该研究旨在比较无症状严重左心室(LV)功能障碍和冠状动脉疾病(CAD)患者接受冠状动脉搭桥手术(CABG)或经皮冠状动脉介入治疗(PCI)的临床疗效:2007年2月至2020年2月期间,共有745名患者因左心室射血分数(LVEF)降低而接受冠状动脉造影检查,这些患者被诊断为扩张型心肌病或无冠状动脉狭窄的瓣膜性心脏病,既往有CABG或瓣膜手术史(59人)、排除了ST段抬高型心肌梗死(STEMI)患者、患有CAD且SYNTAX评分≦22分的患者(175人)、因冠状动脉穿孔而接受紧急CABG手术的患者(3人)以及NYHA分级≦2级的患者(65人)。最后,本研究招募了116名LVEF降低和SYNTAX评分>22的患者,他们分别接受了CABG(47人)和PCI(69人):院内病程、院内死亡率、急性肾损伤和术后血液透析的发生率无明显差异。两组随访 1 年的复发性心肌梗死、血管重建或中风发生率无明显差异。CABG组的1年心衰(HF)住院率明显低于PCI组的所有患者(13.2% vs. 33.3%; p = 0.035);然而,CABG组与完全血管再通亚组在同一变量上没有明显差异(13.2% vs. 28.2%; p = 0.160)。CABG组的血管再通指数(RI)明显高于PCI组或完全血管再通亚组的所有患者(0.93 ± 0.12 vs. 0.71 ± 0.25; p < 0.001)和(0.93 ± 0.12 vs. 0.86 ± 0.13; p = 0.019)。CABG组患者的3年HF住院率明显低于PCI组的所有患者(16.2% vs. 42.2%;p = 0.008);然而,CABG组与完全血运重建亚组之间在同一变量上没有差异(16.2% vs. 35.1%;p = 0.109):结论:对于有症状(NYHA分级≥3级)的严重左心室功能障碍和CAD患者,与PCI组患者相比,CABG手术带来的HF入院率更低,但与完全血管再通亚组患者相比没有差异。因此,在此类人群中,通过 CABG 或 PCI 实现的广泛血管再通与 3 年随访期间较低的 HF 住院率有关。
期刊介绍:
Cardiology Research and Practice is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies that focus on the diagnosis and treatment of cardiovascular disease. The journal welcomes submissions related to systemic hypertension, arrhythmia, congestive heart failure, valvular heart disease, vascular disease, congenital heart disease, and cardiomyopathy.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


