{"title":"Griseofulvin-Induced Red and Hot Ears","authors":"Anand Mannu MD, Abhinav Kumar Verma MD, Biju Vasudevan MD, Pankaj Das MD, Lekshmipriya Krishnan MD","doi":"10.1002/jcph.2383","DOIUrl":null,"url":null,"abstract":"<p>Dear Editor,</p><p>Griseofulvin is a natural product, first isolated in 1939 from <i>Penicillium griseofulvum</i> and was first commercially introduced in 1959. It is a polyketide that is derived from acetyl and malonyl coenzyme A precursor molecules to form dehydrogriseofulvin.<span><sup>1</sup></span> It inhibits microtubule assembly, affects the formation of the mitotic spindle, and finally inhibits mitosis in dermatophytes.<span><sup>2</sup></span> Griseofulvin is mainly used for dermatophytes; however, other uses include anti-inflammatory, cardiovascular, antitumor, and antiviral activity.<span><sup>3</sup></span> It has mainly gastrointestinal side effects, but other adverse effects can also be noticed, such as photosensitivity, urticaria, and petechia.<span><sup>4</sup></span></p><p>A 45-year-old woman with no known comorbidities presented with complaints of multiple itchy, erythematous annular plaques with central clearing over the lower back and gluteal region for the past month, which was diagnosed as tinea corporis, as a potassium hydroxide mount of skin scraping showed fungal hyphae. She was started on oral griseofulvin 500 mg once daily along with topical clotrimazole cream. After 3 days of treatment, she developed swelling and redness in both ears associated with mild pain and itching. There was no history of trauma, fever, sore throat, ear piercing, otorrhea, swimming, topical application, or any other drug intake except griseofulvin and no history of similar episodes or consumption of griseofulvin in the past. On examination, there was diffuse swelling and erythema of the bilateral pinna also involving the lobules (Figure 1). Warmth and tenderness were present. There was no localized abscess formation and no sign of any trauma, wounds, or lymphadenopathy noted. The otoscopy examination was within normal limits.</p><p>Differential diagnosis of erysipelas, cellulitis, otitis externa, relapsing polychondritis, perichondritis, flushing, photosensitivity, seborrheic dermatitis, and red ear syndrome was made as no fever, swollen lymph nodes or trauma, and involvement of bilateral ears at the first episode with normal blood investigations ruled out above differentials. Griseofulvin was suspected as the culprit drug, which was stopped, and she was prescribed a short course of oral prednisolone 40 mg once daily for 5 days along with emollients. After 5 days of treatment, her symptoms subsided with near complete resolution of erythema and swelling (Figure 2). The itching and pain also subsided. For further confirmation of this adverse effect of the drug, griseofulvin was readministered as a single dose, and the patient developed a similar reaction within 24 hours. Laboratory tests for concentration in blood or other fluids were not done as the facility was not available. There were no alternative causes found for such a reaction. Her Naranjo Scale score was 8, which falls under the “probable” category of adverse drug reaction probability scale (Table 1).</p><p>Griseofulvin is a commonly used oral antifungal and is available in 2 forms, micro-size and ultra-micro-size, with the absorption of the latter being better. Common adverse effects of griseofulvin include nausea, vomiting, and diarrhea.<span><sup>5</sup></span> Other adverse effects include photosensitivity, fixed drug eruption, and urticaria. Photosensitivity limited to ears may be one reason in our case, which is not reported. This finding did not fit in any classical benign cutaneous adverse drug reactions. Red ear syndrome is characterized by multiple episodes of unilateral or bilateral erythema and burning sensation lasting minutes to hours. It may be idiopathic or secondary to trigeminal autonomic cephalalgias or migraine. Common triggers to red ear syndrome are heat, cold, chewing, or exertion.<span><sup>6</sup></span> Griseofulvin may be a trigger for red ear syndrome, which has not been studied. We are the first to report bilateral red and hot ears as adverse reactions probably due to oral griseofulvin.</p><p>A.M.: Concept, design of the work; acquisition, analysis, interpretation of data for the work, and drafting. A.K.V.: Concept, design of the work; acquisition, analysis, interpretation of data for the work, and drafting. B.V.: Concept, design of the work; acquisition, analysis, interpretation of data for the work, and drafting. P.D.: Concept, design of the work; acquisition, analysis, interpretation of data for the work, and drafting. L.K.: Concept, design of the work; acquisition, analysis, interpretation of data for the work, and drafting.</p><p>The authors declare no conflicts of interest.</p><p>Written and verbal informed consent for usage of images in publication have been properly obtained from the patient.</p>","PeriodicalId":22751,"journal":{"name":"The Journal of Clinical Pharmacology","volume":null,"pages":null},"PeriodicalIF":0.0000,"publicationDate":"2023-11-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jcph.2383","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Journal of Clinical Pharmacology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jcph.2383","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Dear Editor,
Griseofulvin is a natural product, first isolated in 1939 from Penicillium griseofulvum and was first commercially introduced in 1959. It is a polyketide that is derived from acetyl and malonyl coenzyme A precursor molecules to form dehydrogriseofulvin.1 It inhibits microtubule assembly, affects the formation of the mitotic spindle, and finally inhibits mitosis in dermatophytes.2 Griseofulvin is mainly used for dermatophytes; however, other uses include anti-inflammatory, cardiovascular, antitumor, and antiviral activity.3 It has mainly gastrointestinal side effects, but other adverse effects can also be noticed, such as photosensitivity, urticaria, and petechia.4
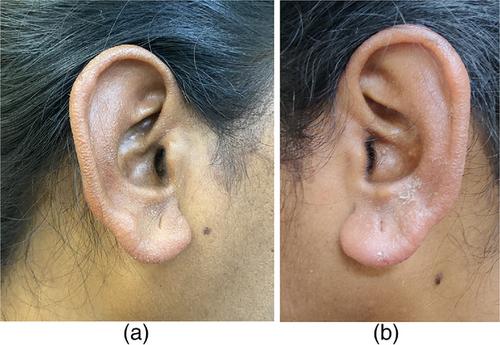
A 45-year-old woman with no known comorbidities presented with complaints of multiple itchy, erythematous annular plaques with central clearing over the lower back and gluteal region for the past month, which was diagnosed as tinea corporis, as a potassium hydroxide mount of skin scraping showed fungal hyphae. She was started on oral griseofulvin 500 mg once daily along with topical clotrimazole cream. After 3 days of treatment, she developed swelling and redness in both ears associated with mild pain and itching. There was no history of trauma, fever, sore throat, ear piercing, otorrhea, swimming, topical application, or any other drug intake except griseofulvin and no history of similar episodes or consumption of griseofulvin in the past. On examination, there was diffuse swelling and erythema of the bilateral pinna also involving the lobules (Figure 1). Warmth and tenderness were present. There was no localized abscess formation and no sign of any trauma, wounds, or lymphadenopathy noted. The otoscopy examination was within normal limits.
Differential diagnosis of erysipelas, cellulitis, otitis externa, relapsing polychondritis, perichondritis, flushing, photosensitivity, seborrheic dermatitis, and red ear syndrome was made as no fever, swollen lymph nodes or trauma, and involvement of bilateral ears at the first episode with normal blood investigations ruled out above differentials. Griseofulvin was suspected as the culprit drug, which was stopped, and she was prescribed a short course of oral prednisolone 40 mg once daily for 5 days along with emollients. After 5 days of treatment, her symptoms subsided with near complete resolution of erythema and swelling (Figure 2). The itching and pain also subsided. For further confirmation of this adverse effect of the drug, griseofulvin was readministered as a single dose, and the patient developed a similar reaction within 24 hours. Laboratory tests for concentration in blood or other fluids were not done as the facility was not available. There were no alternative causes found for such a reaction. Her Naranjo Scale score was 8, which falls under the “probable” category of adverse drug reaction probability scale (Table 1).
Griseofulvin is a commonly used oral antifungal and is available in 2 forms, micro-size and ultra-micro-size, with the absorption of the latter being better. Common adverse effects of griseofulvin include nausea, vomiting, and diarrhea.5 Other adverse effects include photosensitivity, fixed drug eruption, and urticaria. Photosensitivity limited to ears may be one reason in our case, which is not reported. This finding did not fit in any classical benign cutaneous adverse drug reactions. Red ear syndrome is characterized by multiple episodes of unilateral or bilateral erythema and burning sensation lasting minutes to hours. It may be idiopathic or secondary to trigeminal autonomic cephalalgias or migraine. Common triggers to red ear syndrome are heat, cold, chewing, or exertion.6 Griseofulvin may be a trigger for red ear syndrome, which has not been studied. We are the first to report bilateral red and hot ears as adverse reactions probably due to oral griseofulvin.
A.M.: Concept, design of the work; acquisition, analysis, interpretation of data for the work, and drafting. A.K.V.: Concept, design of the work; acquisition, analysis, interpretation of data for the work, and drafting. B.V.: Concept, design of the work; acquisition, analysis, interpretation of data for the work, and drafting. P.D.: Concept, design of the work; acquisition, analysis, interpretation of data for the work, and drafting. L.K.: Concept, design of the work; acquisition, analysis, interpretation of data for the work, and drafting.
The authors declare no conflicts of interest.
Written and verbal informed consent for usage of images in publication have been properly obtained from the patient.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


