Adam Gade Ellesøe, Rawand Shado, Ines Novo Pereira, David Madruga, Haidar Hassan
{"title":"Soft tissue expansion using self-inflating osmotic hydrogel expanders prior to bone augmentation: healing and complications. Evidence-based review.","authors":"Adam Gade Ellesøe, Rawand Shado, Ines Novo Pereira, David Madruga, Haidar Hassan","doi":"10.1038/s41405-023-00175-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>This review aims to assess complication rates, soft tissue gain, and bone gain associated with the use of self-inflating osmotic hydrogel tissue expanders (SOHTEs) for soft tissue expansion (STE).</p><p><strong>Methods: </strong>A comprehensive search on Pubmed and Google Scholar databases was conducted to identify human studies using SOHTEs for STE; last searched in March 2023. Expansion phase details and expander variables were documented. Complication rates, soft tissue gain, and bone gain reported in each study were also recorded. The inclusion criteria encompassed human studies ranging from evidence levels II-IV (Oxford Centre for Evidence-Based Medicine Levels of Evidence), without specific date limits. For assessing bias in randomized controlled trials (RCTs), a Risk of Bias tool was employed. The synthesised results were presented through tables, sunburst plots, and bar charts.</p><p><strong>Results: </strong>A total of 13 studies were identified, comprising 4 RCTs, 1 cohort study, and 8 case-series. Employment of SOHTEs yielded an overall complication rate of 17% (24/140 sites), with expander perforation accounting for 9.3% (13/140) of the sites. Specific complication rates included dehiscence (1.4%, 2/140 sites), paraesthesia (1.4%, 2/140 sites), and infection (1.4%, 2/140 sites). All randomized controlled trials (RCTs) were categorised at Level II. The remaining investigations primarily consisted of Level IV case-series lacking controls. All studies demonstrated some concerns towards bias.</p><p><strong>Conclusion: </strong>STE studies using SOHTEs exhibit a reduction in complications associated with bone augmentation in scenarios of inadequate soft tissue coverage. Preliminary evidence suggests potential benefits even in cases with sufficient soft tissue. Adherence to procedural precautions may reduce the risk of expander perforations, further diminishing complications. Subsequent studies should incorporate individual patient and expander variables in their reports to explore the impact of expansion phases on complication rates, as well as bone and soft tissue augmentation.</p>","PeriodicalId":36997,"journal":{"name":"BDJ Open","volume":null,"pages":null},"PeriodicalIF":2.5000,"publicationDate":"2023-11-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10640575/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BDJ Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1038/s41405-023-00175-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: This review aims to assess complication rates, soft tissue gain, and bone gain associated with the use of self-inflating osmotic hydrogel tissue expanders (SOHTEs) for soft tissue expansion (STE).
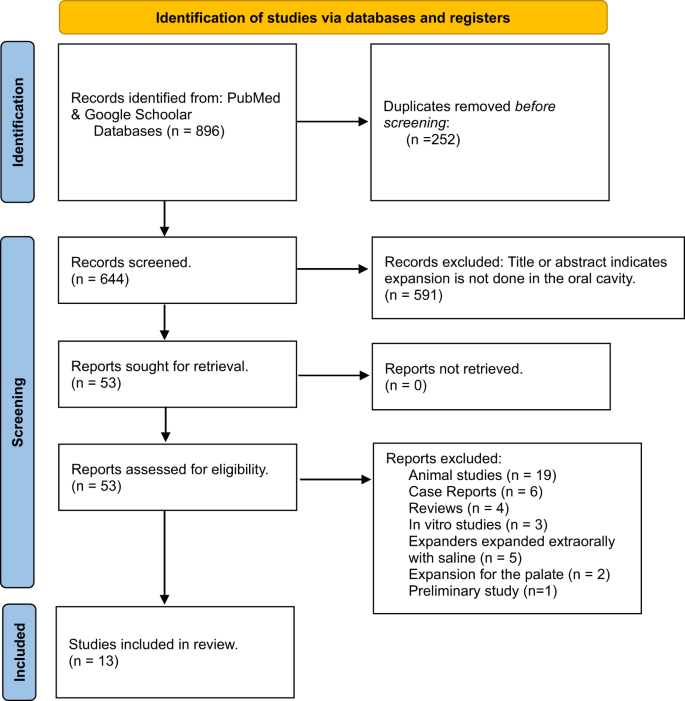
Methods: A comprehensive search on Pubmed and Google Scholar databases was conducted to identify human studies using SOHTEs for STE; last searched in March 2023. Expansion phase details and expander variables were documented. Complication rates, soft tissue gain, and bone gain reported in each study were also recorded. The inclusion criteria encompassed human studies ranging from evidence levels II-IV (Oxford Centre for Evidence-Based Medicine Levels of Evidence), without specific date limits. For assessing bias in randomized controlled trials (RCTs), a Risk of Bias tool was employed. The synthesised results were presented through tables, sunburst plots, and bar charts.
Results: A total of 13 studies were identified, comprising 4 RCTs, 1 cohort study, and 8 case-series. Employment of SOHTEs yielded an overall complication rate of 17% (24/140 sites), with expander perforation accounting for 9.3% (13/140) of the sites. Specific complication rates included dehiscence (1.4%, 2/140 sites), paraesthesia (1.4%, 2/140 sites), and infection (1.4%, 2/140 sites). All randomized controlled trials (RCTs) were categorised at Level II. The remaining investigations primarily consisted of Level IV case-series lacking controls. All studies demonstrated some concerns towards bias.
Conclusion: STE studies using SOHTEs exhibit a reduction in complications associated with bone augmentation in scenarios of inadequate soft tissue coverage. Preliminary evidence suggests potential benefits even in cases with sufficient soft tissue. Adherence to procedural precautions may reduce the risk of expander perforations, further diminishing complications. Subsequent studies should incorporate individual patient and expander variables in their reports to explore the impact of expansion phases on complication rates, as well as bone and soft tissue augmentation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


