Manjri Garg, Jyotsna Sen, Sandeep Goyal, Dhruva Chaudhry
{"title":"Comparative evaluation of central venous pressure and sonographic inferior vena cava variability in assessing fluid responsiveness in septic shock.","authors":"Manjri Garg, Jyotsna Sen, Sandeep Goyal, Dhruva Chaudhry","doi":"10.4103/0972-5229.195706","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Fluid infusion, the most critical step in the resuscitation of patients with septic shock, needs preferably continuous invasive hemodynamic monitoring. The study was planned to evaluate the efficacy of ultrasonographically measured inferior vena cava collapsibility index (IVC CI) in comparison to central venous pressure (CVP) in predicting fluid responsiveness in septic shock.</p><p><strong>Materials and methods: </strong>Thirty-six patients of septic shock requiring ventilatory support (invasive/noninvasive) were included. Patients with congestive heart failure, raised intra-abdominal pressure, and poor echo window were excluded from the study. They were randomly divided into two groups based on mode of fluid resuscitation - Group I (CVP) and Group II (IVC CI). Primary end-points were mean arterial pressure (MAP) of ≥65 mmHg and CVP >12 mmHg or IVC CI <20% in Groups I and II, respectively. Patients were followed till achievement of end-points or maximum of 6 h. Outcome variables (pulse rate, MAP, urine output, pH, base deficit, and ScvO<sub>2</sub> ) were serially measured till the end of the study. Survival at 2 and 4 weeks was used as secondary end-point.</p><p><strong>Results: </strong>Primary end-point was reached in 31 patients (15 in Group I and 16 in Group II). Fluid infusion, by either method, had increased CVP and decreased IVC CI with resultant negative correlation between them (Pearson correlation coefficient -0.626). There was no significant difference in the amount of fluid infused and time to reach end-point in two groups. Comparison in outcome variables at baseline and end-point showed no significant difference including mortality.</p><p><strong>Conclusion: </strong>CVP and IVC CI are negatively correlated with fluid resuscitation, and both methods can be used for resuscitation, with IVC CI being noninferior to CVP.</p>","PeriodicalId":49658,"journal":{"name":"Progress of Theoretical Physics","volume":"82 1","pages":"708-713"},"PeriodicalIF":0.0000,"publicationDate":"2016-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5225771/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Progress of Theoretical Physics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/0972-5229.195706","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
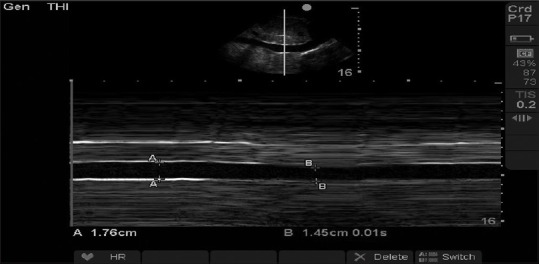
Objective: Fluid infusion, the most critical step in the resuscitation of patients with septic shock, needs preferably continuous invasive hemodynamic monitoring. The study was planned to evaluate the efficacy of ultrasonographically measured inferior vena cava collapsibility index (IVC CI) in comparison to central venous pressure (CVP) in predicting fluid responsiveness in septic shock.
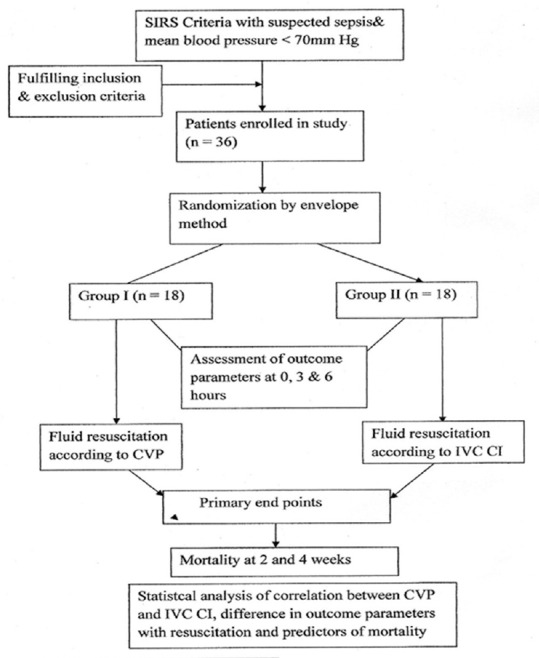
Materials and methods: Thirty-six patients of septic shock requiring ventilatory support (invasive/noninvasive) were included. Patients with congestive heart failure, raised intra-abdominal pressure, and poor echo window were excluded from the study. They were randomly divided into two groups based on mode of fluid resuscitation - Group I (CVP) and Group II (IVC CI). Primary end-points were mean arterial pressure (MAP) of ≥65 mmHg and CVP >12 mmHg or IVC CI <20% in Groups I and II, respectively. Patients were followed till achievement of end-points or maximum of 6 h. Outcome variables (pulse rate, MAP, urine output, pH, base deficit, and ScvO2 ) were serially measured till the end of the study. Survival at 2 and 4 weeks was used as secondary end-point.
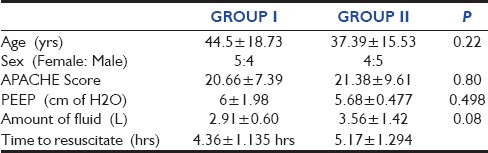
Results: Primary end-point was reached in 31 patients (15 in Group I and 16 in Group II). Fluid infusion, by either method, had increased CVP and decreased IVC CI with resultant negative correlation between them (Pearson correlation coefficient -0.626). There was no significant difference in the amount of fluid infused and time to reach end-point in two groups. Comparison in outcome variables at baseline and end-point showed no significant difference including mortality.
Conclusion: CVP and IVC CI are negatively correlated with fluid resuscitation, and both methods can be used for resuscitation, with IVC CI being noninferior to CVP.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


