{"title":"A nanovesicle platform to deliver neoantigens and immune checkpoint inhibitors: To ASPIRE for novel cancer vaccines","authors":"Hongwei Cheng, Hwan-Ching Tai","doi":"10.1002/mba2.4","DOIUrl":null,"url":null,"abstract":"<p>Tumor immunotherapy has made a breakthrough in clinical application, and the combination of vaccine and immune checkpoint inhibitors (ICI) is a promising strategy in cancer management. However, the complete immune response is still unresolved. Liu et al.<span><sup>1</sup></span> report a genetically engineered cell membrane nanovesicle, which integrates antigen self-presentation and immunosuppression reversal (ASPIRE) for boosting cancer immunotherapy (Figure 1). It is the comprehensive demonstration of a personalized vaccine formula that has the power to directly activate both naive T cells and exhausted T cells. Besides, this artificial nanovaccine has a nanoscale size, better stability, and an excellent homing effect, which could rapidly enrich the lymphatic system. This specific antigen self-presentation strategy is superior to conventional vaccines. Importantly, B7 codelivery is first introduced to the anti-PD1 therapy, which not only activates T lymphocyte immune response but also breaks immunosuppression.</p><p>In 1971, the US government declared a “war on cancer” through its National Cancer Act, which marked the beginning of modern cancer research. Half a century later, despite significant progress in many areas of cancer treatment, cancer remains a leading cause of death globally. Therefore, the quest to search for new and creative ways to cure cancer continues. A new strategy that has attracted much attention is to train or augment our own immune system to destroy cancer cells. The feasibility of this idea has been recently demonstrated through the clinical successes of ICI, such as anti-PD-1 or anti-PDL1 antibodies, and chimeric antigen receptor (CAR) T-cell therapies.<span><sup>2</sup></span></p><p>However, the clinical benefits of ICI and CAR T-cell therapies are still relatively limited compared to conventional chemotherapies or targeted therapies based on small-molecule drugs. Although our immune system has the capacity to target cancer cells, there are also various ways that cancer cells may evolve to escape such immune surveillance. After all, cancer cells originate from our own somatic cells, which have various ways to avoid being attacked by the immune system. There is a need for more efficient and more widely applicable methods to boost immune defenses against various types of cancers, and the idea of vaccination naturally comes to mind.</p><p>Even before we had any scientific understanding of the pathogens causing infectious diseases or the inner workings of immune systems, the first modern vaccine (against smallpox) was successfully developed by the end of the 18th century. A dozen vaccines were developed before the Second World War, before the breakthrough discoveries in molecular biology. Then, why not develop vaccines for certain types of cancer?</p><p>It turns out that we cannot vaccinate against tumors simply by the systematic administration of antigens found on cancer cells. Through recent research into the tumor microenvironment, we began to realize that a special group of antigen-presenting cells called dendritic cells (DCs) play key regulatory roles in cancer-related immunity.<span><sup>3</sup></span> DCs present tumor-associated antigens to CD8+ (cytotoxic) T cells, CD4+ T cells, and B cells to activate the adaptive immune responses. The working principle of ICI is to block the inhibitory communications between DCs and T cells, thereby favoring T cell activation. Thus, a new generation of cancer vaccine technologies now focuses on the activation or utilization of DCs to present tumor-related antigens.</p><p>The communication between DCs and T cells involves many molecular recognition events, including: (1) antigen presentation on major histocompatibility complexes (MHCs) and their recognition by T cell receptors; (2) costimulation signals involving membrane proteins on DCs (e.g., B7-1/CD80) interacting with membrane proteins on T cells (e.g., CD28), although some interactions are inhibitory, such as those between PDL1 and PD1; (3) released cytokines signaling through plasma membrane receptors.<span><sup>3</sup></span> Hence, DCs loaded ex vivo with tumor-related antigens may be reintroduced into the body as a cancer vaccine.<span><sup>4</sup></span> From a reductionist point of view, one may consider the DC as a platform for presenting a wide variety of molecular signals. One may also wonder if such a signaling platform could also function in the absence of living cells, which has led to the development of vaccines based on DC-derived vesicles. A new study by Liu et al.<span><sup>1</sup></span> has explored novel strategies to construct a nanovesicle cancer vaccine platform that could deliver multiple immune-modulatory signals without involving live DCs.</p><p>This novel nanovaccine platform has been termed ASPIRE, which stands for antigen self-presentation and immunosuppression reversal. It involved the ex vivo engineering of DCs via a two-step process. First, they were transfected with a plasmid to express a surface membrane protein carrying the anti-PD1 single-chain variable fragment antibody. This created an ICI displayed on the plasma membrane to block immunosuppression. Second, the presentation of neoantigens was achieved by infecting DCs with recombinant adenovirus vectors, which resulted in the surface presentation of multiple antigenic peptides on MHC-I (Figure 1A). The viral infection also stimulated the surface expression of CD80 (B7-1) and CD86 (B7-2), which could bind to CD28 on T cell surfaces to stimulate the immune response (Figure 1B). The engineered DCs were disrupted by sonication, and the nanovesicles derived from plasma membranes were collected by sucrose gradient centrifugation. The biomimetic APSIRE nanovaccine may be viewed as the reorganized plasma membrane of antigen-presenting DCs supplemented with surface-bound ICI.</p><p>The authors first demonstrated the capacity of ASPIRE nanovaccines to stimulate CD8+ T cells both ex vivo and in vivo. The nanoscale size, good stability, and homing effects ensured the rapid enrichment of ASPIRE nanovaccines in the lymph nodes, where DCs would normally stimulate T cells (Figure 1C). They also observed that the presence of CD80 and CD86 are important factors in ensuring robust T cell activation.</p><p>Next, the authors tried to evaluate the antitumor effects of ASPIRE nanovaccine using a mouse melanoma model. Previous clinical studies have shown that multi-neoantigen long-peptide vaccines or multiantigen liposome-RNA vaccines can work synergistically with anti-PD1 ICI therapy in melanoma patients.<span><sup>5</sup></span> Therefore, the combination of multi-antigen cancer vaccine and ICI appears to be a promising strategy against melanomas. To mimic such a combination, Liu et al. expressed multiple melanoma neoantigens on DCs as well as membrane-bound PD1 antibody fragments, and it turned out to be highly effective in treating mouse melanoma models.</p><p>In summary, the ASPIRE nanovaccine is an ingenious platform for stimulating the adaptive immune response of cytotoxic T cells. It is not yet clear how the efficacy of ASPIRE nanovaccines compares with that of engineered DC vaccines. The obvious advantages of nanovesicle vaccines over cellular vaccines include stability and ease of storage. Moreover, the much smaller size of nanovaccines has the potential benefit of deeper penetration into various tissues, entering some tight spaces that may not be accessible by DCs. ASPIRE represents a new way to design and construct multifunctional biomimetic nanoparticle vaccines and holds promising clinical translation potential.</p><p>Hongwei Cheng and Hwan-Ching Tai wrote the original draft. Hwan-Ching Tai reviewed and edited the manuscript. Both authors agreed to submit the final version of the article.</p><p>The authors declare no conflict of interest.</p><p>Ethical approval is not applicable for this article.</p>","PeriodicalId":100901,"journal":{"name":"MedComm – Biomaterials and Applications","volume":"1 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-07-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/mba2.4","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"MedComm – Biomaterials and Applications","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/mba2.4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Tumor immunotherapy has made a breakthrough in clinical application, and the combination of vaccine and immune checkpoint inhibitors (ICI) is a promising strategy in cancer management. However, the complete immune response is still unresolved. Liu et al.1 report a genetically engineered cell membrane nanovesicle, which integrates antigen self-presentation and immunosuppression reversal (ASPIRE) for boosting cancer immunotherapy (Figure 1). It is the comprehensive demonstration of a personalized vaccine formula that has the power to directly activate both naive T cells and exhausted T cells. Besides, this artificial nanovaccine has a nanoscale size, better stability, and an excellent homing effect, which could rapidly enrich the lymphatic system. This specific antigen self-presentation strategy is superior to conventional vaccines. Importantly, B7 codelivery is first introduced to the anti-PD1 therapy, which not only activates T lymphocyte immune response but also breaks immunosuppression.
In 1971, the US government declared a “war on cancer” through its National Cancer Act, which marked the beginning of modern cancer research. Half a century later, despite significant progress in many areas of cancer treatment, cancer remains a leading cause of death globally. Therefore, the quest to search for new and creative ways to cure cancer continues. A new strategy that has attracted much attention is to train or augment our own immune system to destroy cancer cells. The feasibility of this idea has been recently demonstrated through the clinical successes of ICI, such as anti-PD-1 or anti-PDL1 antibodies, and chimeric antigen receptor (CAR) T-cell therapies.2
However, the clinical benefits of ICI and CAR T-cell therapies are still relatively limited compared to conventional chemotherapies or targeted therapies based on small-molecule drugs. Although our immune system has the capacity to target cancer cells, there are also various ways that cancer cells may evolve to escape such immune surveillance. After all, cancer cells originate from our own somatic cells, which have various ways to avoid being attacked by the immune system. There is a need for more efficient and more widely applicable methods to boost immune defenses against various types of cancers, and the idea of vaccination naturally comes to mind.
Even before we had any scientific understanding of the pathogens causing infectious diseases or the inner workings of immune systems, the first modern vaccine (against smallpox) was successfully developed by the end of the 18th century. A dozen vaccines were developed before the Second World War, before the breakthrough discoveries in molecular biology. Then, why not develop vaccines for certain types of cancer?
It turns out that we cannot vaccinate against tumors simply by the systematic administration of antigens found on cancer cells. Through recent research into the tumor microenvironment, we began to realize that a special group of antigen-presenting cells called dendritic cells (DCs) play key regulatory roles in cancer-related immunity.3 DCs present tumor-associated antigens to CD8+ (cytotoxic) T cells, CD4+ T cells, and B cells to activate the adaptive immune responses. The working principle of ICI is to block the inhibitory communications between DCs and T cells, thereby favoring T cell activation. Thus, a new generation of cancer vaccine technologies now focuses on the activation or utilization of DCs to present tumor-related antigens.
The communication between DCs and T cells involves many molecular recognition events, including: (1) antigen presentation on major histocompatibility complexes (MHCs) and their recognition by T cell receptors; (2) costimulation signals involving membrane proteins on DCs (e.g., B7-1/CD80) interacting with membrane proteins on T cells (e.g., CD28), although some interactions are inhibitory, such as those between PDL1 and PD1; (3) released cytokines signaling through plasma membrane receptors.3 Hence, DCs loaded ex vivo with tumor-related antigens may be reintroduced into the body as a cancer vaccine.4 From a reductionist point of view, one may consider the DC as a platform for presenting a wide variety of molecular signals. One may also wonder if such a signaling platform could also function in the absence of living cells, which has led to the development of vaccines based on DC-derived vesicles. A new study by Liu et al.1 has explored novel strategies to construct a nanovesicle cancer vaccine platform that could deliver multiple immune-modulatory signals without involving live DCs.
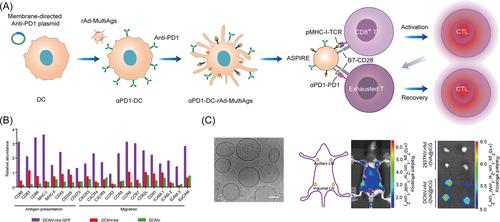
This novel nanovaccine platform has been termed ASPIRE, which stands for antigen self-presentation and immunosuppression reversal. It involved the ex vivo engineering of DCs via a two-step process. First, they were transfected with a plasmid to express a surface membrane protein carrying the anti-PD1 single-chain variable fragment antibody. This created an ICI displayed on the plasma membrane to block immunosuppression. Second, the presentation of neoantigens was achieved by infecting DCs with recombinant adenovirus vectors, which resulted in the surface presentation of multiple antigenic peptides on MHC-I (Figure 1A). The viral infection also stimulated the surface expression of CD80 (B7-1) and CD86 (B7-2), which could bind to CD28 on T cell surfaces to stimulate the immune response (Figure 1B). The engineered DCs were disrupted by sonication, and the nanovesicles derived from plasma membranes were collected by sucrose gradient centrifugation. The biomimetic APSIRE nanovaccine may be viewed as the reorganized plasma membrane of antigen-presenting DCs supplemented with surface-bound ICI.
The authors first demonstrated the capacity of ASPIRE nanovaccines to stimulate CD8+ T cells both ex vivo and in vivo. The nanoscale size, good stability, and homing effects ensured the rapid enrichment of ASPIRE nanovaccines in the lymph nodes, where DCs would normally stimulate T cells (Figure 1C). They also observed that the presence of CD80 and CD86 are important factors in ensuring robust T cell activation.
Next, the authors tried to evaluate the antitumor effects of ASPIRE nanovaccine using a mouse melanoma model. Previous clinical studies have shown that multi-neoantigen long-peptide vaccines or multiantigen liposome-RNA vaccines can work synergistically with anti-PD1 ICI therapy in melanoma patients.5 Therefore, the combination of multi-antigen cancer vaccine and ICI appears to be a promising strategy against melanomas. To mimic such a combination, Liu et al. expressed multiple melanoma neoantigens on DCs as well as membrane-bound PD1 antibody fragments, and it turned out to be highly effective in treating mouse melanoma models.
In summary, the ASPIRE nanovaccine is an ingenious platform for stimulating the adaptive immune response of cytotoxic T cells. It is not yet clear how the efficacy of ASPIRE nanovaccines compares with that of engineered DC vaccines. The obvious advantages of nanovesicle vaccines over cellular vaccines include stability and ease of storage. Moreover, the much smaller size of nanovaccines has the potential benefit of deeper penetration into various tissues, entering some tight spaces that may not be accessible by DCs. ASPIRE represents a new way to design and construct multifunctional biomimetic nanoparticle vaccines and holds promising clinical translation potential.
Hongwei Cheng and Hwan-Ching Tai wrote the original draft. Hwan-Ching Tai reviewed and edited the manuscript. Both authors agreed to submit the final version of the article.
The authors declare no conflict of interest.
Ethical approval is not applicable for this article.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


