Aleksandra Sucharska, Agnieszka Adamowska, Zuzanna Karbowska, Lavanya Mohan Kumar, Jakub Pudełko, Łukasz Szarpak, Marek Jemielity, Bartłomiej Perek
{"title":"Do we correctly calculate doses of cardioplegia during aortic valve replacement procedures? A preliminary report.","authors":"Aleksandra Sucharska, Agnieszka Adamowska, Zuzanna Karbowska, Lavanya Mohan Kumar, Jakub Pudełko, Łukasz Szarpak, Marek Jemielity, Bartłomiej Perek","doi":"10.5114/kitp.2023.130660","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Intraoperative myocardial protection during aortic valve replacement (AVR) for aortic stenosis (AS) is of paramount importance for outcomes. The dose of cardioplegia is usually calculated with reference to body mass.</p><p><strong>Aim: </strong>To assess whether such a strategy should be applied to all AS patients undergoing AVR.</p><p><strong>Material and methods: </strong>The study included 94 patients who underwent elective isolated AVR in cardiopulmonary bypass with cold cardioplegic arrest, with a mean age of 65.4 ±7.8 years. They were divided into two subgroup: A with an infusion of high (above median) and subgroup B with a low (below median) volume of cardioplegia indexed for left ventricular mass (LVM). Their doses were referred to the maximal postoperative release of cardiac troponin I (cTnI max). Eventually, it was examined whether the extent of intraoperative myocardial injury translated into long-term survival stratified according to the Kaplan-Meier method.</p><p><strong>Results: </strong>The mean volume of cardioplegia was 1381 ±279 ml (4.9 ±1.6 ml/g of LV myocardium). cTnI max was much higher in group A than in group B (medians: 14.918 vs. 9.876 μg/l; <i>p</i> = 0.005). Moreover, a negative correlation between the index cardioplegia volume and cTnI max (<i>r</i> = 0.345) was noted. The five-year probability of survival in subgroup A (95.7%) was significantly better than that in subgroup B individuals (82.6%, <i>p</i> = 0.044).</p><p><strong>Conclusions: </strong>Calculating cardioplegic doses during AVR solely based on body mass may be suboptimal and have a significant impact on postoperative outcomes.</p>","PeriodicalId":49945,"journal":{"name":"Kardiochirurgia I Torakochirurgia Polska","volume":"20 3","pages":"155-160"},"PeriodicalIF":0.6000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10626402/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kardiochirurgia I Torakochirurgia Polska","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/kitp.2023.130660","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/11 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Intraoperative myocardial protection during aortic valve replacement (AVR) for aortic stenosis (AS) is of paramount importance for outcomes. The dose of cardioplegia is usually calculated with reference to body mass.
Aim: To assess whether such a strategy should be applied to all AS patients undergoing AVR.
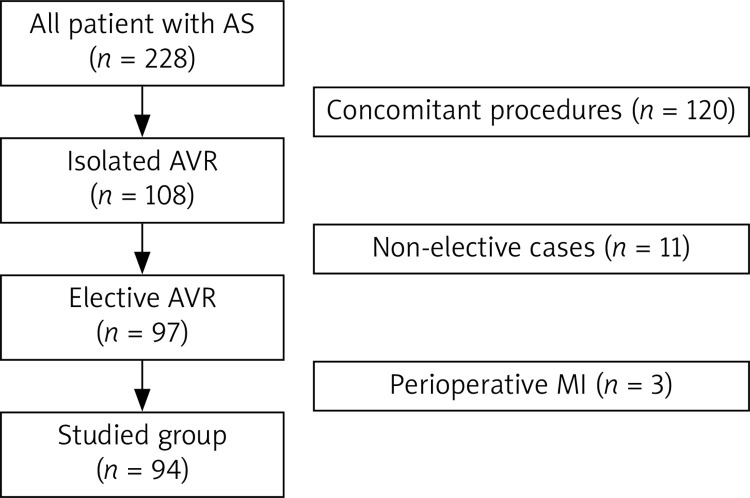
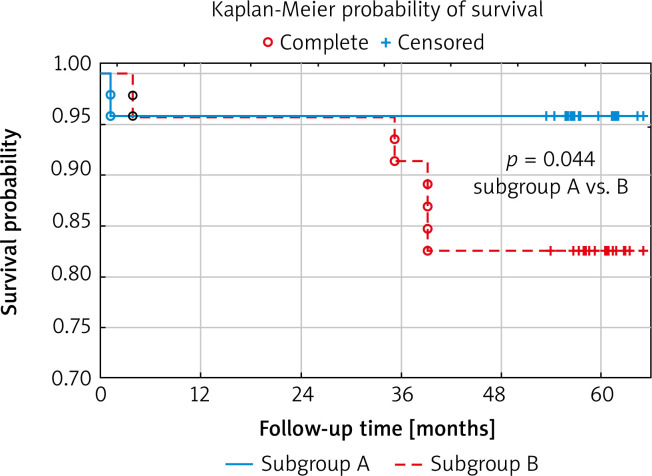
Material and methods: The study included 94 patients who underwent elective isolated AVR in cardiopulmonary bypass with cold cardioplegic arrest, with a mean age of 65.4 ±7.8 years. They were divided into two subgroup: A with an infusion of high (above median) and subgroup B with a low (below median) volume of cardioplegia indexed for left ventricular mass (LVM). Their doses were referred to the maximal postoperative release of cardiac troponin I (cTnI max). Eventually, it was examined whether the extent of intraoperative myocardial injury translated into long-term survival stratified according to the Kaplan-Meier method.
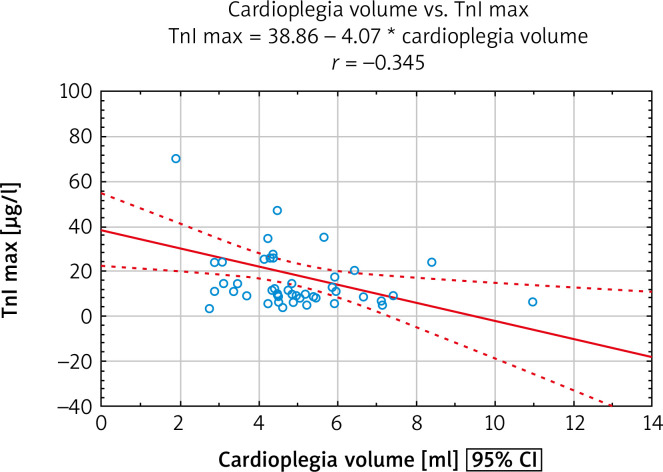
Results: The mean volume of cardioplegia was 1381 ±279 ml (4.9 ±1.6 ml/g of LV myocardium). cTnI max was much higher in group A than in group B (medians: 14.918 vs. 9.876 μg/l; p = 0.005). Moreover, a negative correlation between the index cardioplegia volume and cTnI max (r = 0.345) was noted. The five-year probability of survival in subgroup A (95.7%) was significantly better than that in subgroup B individuals (82.6%, p = 0.044).
Conclusions: Calculating cardioplegic doses during AVR solely based on body mass may be suboptimal and have a significant impact on postoperative outcomes.
期刊介绍:
Polish Journal of Thoracic and Cardiovascular Surgery is a quarterly aimed at cardiologists, cardiosurgeons and thoracic surgeons. Includes the original works (experimental, research and development), illustrative and casuistical works about cardiology and cardiosurgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


